Benzhydrocodone
Severe
Database
Drug interaction classified as: metabolism
Source: DDInter
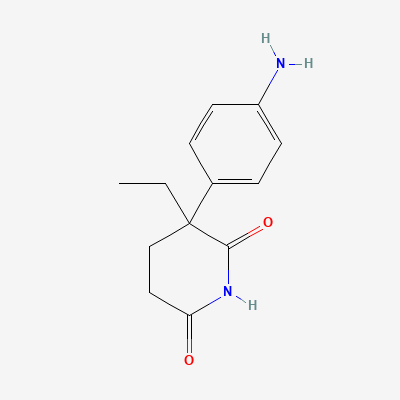
Adrenocortical steroidogenesis inhibitor (historical) · Antineoplastic
KDIGO 2024 + manufacturer label
Inhibits cholesterol side-chain cleavage (CYP11A1) and aromatase (CYP19), suppressing adrenal steroid (cortisol, aldosterone) and peripheral oestrogen synthesis; historical 'medical adrenalectomy' role in Cushing's and metastatic breast cancer.
Contraindicated — virilisation of female fetus.
Avoid.
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Decreased progesterone plasma concentrations, leading to reduced efficacy.
Avoid co-administration. If unavoidable, consider increasing progesterone dose or using an alternative progestin. Monitor for signs of reduced progesterone effect.
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Aminoglutethimide induces dexamethasone metabolism
Use hydrocortisone for replacement instead
Source: Kimi deep-research + Cla
Decreased plasma concentrations and efficacy of medroxyprogesterone acetate, potentially reducing its therapeutic effect.
Monitor for reduced efficacy of medroxyprogesterone acetate. Dose adjustment may be necessary, or consider an alternative progestin.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20