Amisulpride
Contraindicated
Database
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
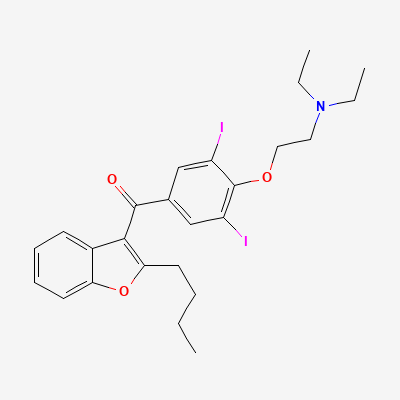
Class III antiarrhythmic (multichannel) · Arrhythmia management
Also known as Amiodarone hydrochloride
KDIGO 2024 + manufacturer label
33 branded formulations. Look up specific brands in the Drugs workspace.
Prolongs action-potential duration/refractoriness via K+ channel blockade, with additional Na+ and Ca2+ channel and non-competitive alpha/beta blockade; broad antiarrhythmic activity. Iodine-rich, highly lipophilic, very long-acting.
Avoid — fetal hypothyroidism/goitre, neurodevelopmental risk; only for life-threatening maternal arrhythmia
Contraindicated — significant excretion in milk, infant thyroid risk
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Additive QT prolongation; high risk of torsades de pointes
Avoid combination; if unavoidable, monitor QTc closely
Source: Kimi deep-research + Cla
Increased risk of Torsades de Pointes (TdP), ventricular arrhythmias, and sudden cardiac death.
Avoid concomitant use. If no alternative exists and co-administration is absolutely necessary, continuous ECG monitoring and electrolyte correction are mandatory, but generally not recommended.
Source: DDInter
Increased antiarrhythmic levels
Contraindicated; choose alternative COVID therapy
Source: Kimi deep-research + Cla
Drug interaction classified as: synergy
Source: DDInter
Plasma levels of CYP2C8 substrates (e.g., amiodarone, carbamazepine, cerivastatin, diclofenac, ibuprofen, paclitaxel, rosiglitazone) may increase.
Requires careful monitoring for toxicity and possibly dose adjustment of the CYP2C8 substrate.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19