Aminoglycosides
Moderate
Database
Synergistic Gram-negative coverage (intended)
Standard combination; monitor renal function
Source: Kimi deep-research + Cla
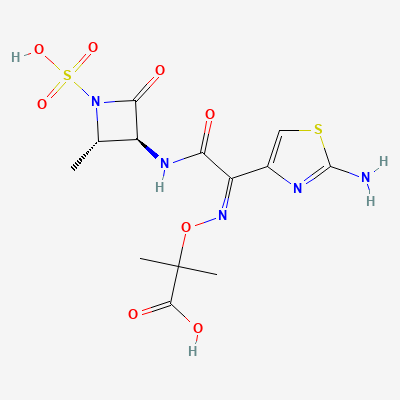
Monobactam (β-lactam) antibiotic · Antibacterial
KDIGO 2024 + manufacturer label
Binds penicillin-binding protein 3 of Gram-negative aerobes, inhibiting bacterial cell-wall synthesis; selective for aerobic Gram-negatives (including Pseudomonas) with no Gram-positive or anaerobic activity.
Considered acceptable when indicated (β-lactam class).
Compatible with breastfeeding.
Synergistic Gram-negative coverage (intended)
Standard combination; monitor renal function
Source: Kimi deep-research + Cla
Shared side chain
Avoid if severe ceftazidime allergy
Source: Kimi deep-research + Cla
Increased risk of renal dysfunction, particularly when aztreonam is co-administered with other nephrotoxic drugs. Loop diuretics can also reduce aztreonam excretion.
Monitor renal function closely. Be aware of potential for reduced aztreonam excretion, which may necessitate dose adjustment in patients with impaired renal function. Avoid concomitant use with other nephrotoxic agents if possible.
Renal stress
Monitor renal function
Source: Kimi deep-research + Cla
Reduced renal tubular secretion
Monitor; usually no adjustment
Source: Kimi deep-research + Cla
Decreased serum concentrations of valproic acid, potentially leading to loss of seizure control.
Monitor valproic acid levels closely. Consider increasing valproic acid dose or switching to an alternative antiepileptic drug if clinically indicated. Monitor for seizure recurrence.
6 additional low-confidence interactions hidden — those rows lack a documented mechanism or management plan in our sources.
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20