Mao Inhibitors
Contraindicated
Database
Risk of hypertensive crisis and CNS effects; brimonidine is an alpha-2 agonist.
Contraindicated. Wait 14 days after MAOI discontinuation before starting brimonidine.
Source: Kimi deep-research + Cla
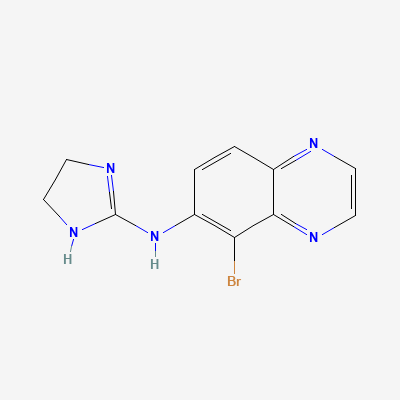
Selective alpha-2 adrenergic receptor agonist · Antiglaucoma agent
Also known as Brimonidine Tartrate, Alphagan P
KDIGO 2024 + manufacturer label
33 branded formulations and 67 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Selective alpha-2 adrenergic agonism reduces aqueous humor production and increases uveoscleral outflow, lowering intraocular pressure. More selective than apraclonidine (less alpha-1 effect = fewer allergic reactions).
Limited data; minimal systemic absorption with ophthalmic use. Use only if benefit outweighs risk.
Excretion in breast milk unknown; minimal systemic absorption suggests low risk. Monitor infant for sedation and dry mouth.
Risk of hypertensive crisis and CNS effects; brimonidine is an alpha-2 agonist.
Contraindicated. Wait 14 days after MAOI discontinuation before starting brimonidine.
Source: Kimi deep-research + Cla
11 additional low-confidence interactions hidden — those rows lack a documented mechanism or management plan in our sources.
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19