Carbamazepine
Severe
Textbook-cited
Reduced chloramphenicol efficacy
Avoid concurrent use or increase dose with monitoring
Source: KDT 7e · p949
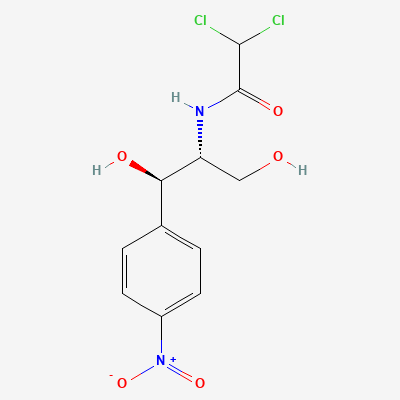
Amphenicol antibiotic / bacteriostatic (bactericidal at high concentrations) · Antibiotic
Also known as Chloromycetin, Chloroptic, Phenicol
KDIGO 2024 + manufacturer label
198 branded formulations and 66 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Reversibly binds to 50S ribosomal subunit, inhibiting bacterial peptidyl transferase and blocking peptide bond formation and protein synthesis. Broad spectrum of activity including Gram-positive, Gram-negative, anaerobes, and atypicals (Rickettsia, Mycoplasma, Chlamydia).
Avoid in pregnancy especially third trimester; risk of gray baby syndrome; only if no safer alternative
Excreted in breast milk; avoid if possible; may cause bone marrow suppression in infant
Reduced chloramphenicol efficacy
Avoid concurrent use or increase dose with monitoring
Source: KDT 7e · p949
Hypoglycemia
Monitor blood glucose; reduce sulfonylurea dose
Source: KDT 7e · p949
Hypoglycemia
Monitor blood glucose; reduce sulfonylurea dose
Source: KDT 7e · p949
Hypoglycemia
Monitor blood glucose; reduce sulfonylurea dose
Source: KDT 7e · p949
Hypoglycemia
Monitor blood glucose; reduce sulfonylurea dose
Source: KDT 7e · p949
Reduced chloramphenicol efficacy
Avoid concurrent use or increase dose with monitoring
Source: KDT 7e · p949
Reduced chloramphenicol efficacy
Avoid concurrent use or increase dose with monitoring
Source: KDT 7e · p949
Prolonged half-lives of drugs metabolized by CYPs.
Recognize this effect to avoid severe toxicity and potentially fatal outcomes.
Source: G&G 14e · p1189
Apparent antagonism on pneumococci; higher mortality in pneumococcal meningitis compared to penicillin alone.
Avoid combination for highly sensitive organisms where cidal drug alone is sufficient.
Source: KDT 7e · p699
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19