Agalsidase Beta
Severe
Database
Drug interaction classified as: antagonism
Source: DDInter
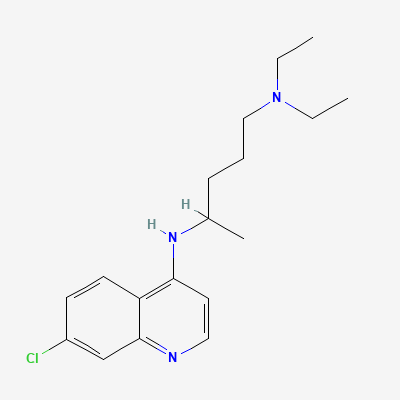
4-aminoquinoline antimalarial / disease-modifying antirheumatic · Antirheumatic
Also known as Chloroquine phosphate, Chloroquine sulfate, Aralen, Resochin, Nivaquine
KDIGO 2024 + manufacturer label
137 branded formulations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
In malaria: concentrates in parasite food vacuole, inhibiting heme polymerization → toxic free heme accumulation → parasite death. In autoimmune disease: inhibits Toll-like receptor signaling, reduces cytokine production, and stabilizes lysosomal membranes.
Safe for malaria prophylaxis and treatment in pregnancy (WHO recommended). For autoimmune disease, lowest effective dose preferred—retinal toxicity risk to fetus theoretical but unproven. Crosses placenta.
Excreted in breast milk in small amounts (~2-3% of maternal dose); compatible with breastfeeding for malaria prophylaxis/treatment per WHO. Infant should receive complementary antimalarial prophylaxis.
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Additive QT prolongation; risk of torsades de pointes and sudden cardiac death.
Avoid combination; if essential, monitor ECG (QTc) closely. Correct electrolytes (K+, Mg2+).
Source: Kimi deep-research + Cla
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19