Linezolid
Contraindicated
Database
Serotonin syndrome risk.
Contraindicated. Use alternative antibiotic.
Source: DDInter
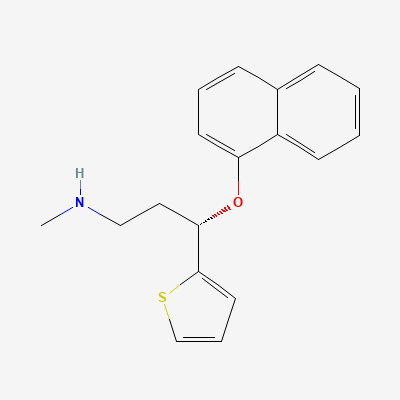
Serotonin-norepinephrine reuptake inhibitor (SNRI) · Antidepressant
Also known as Duloxetine Hydrochloride, Cymbalta, Dulojoy, Duwell, Depralin, Duxet
KDIGO 2024 + manufacturer label
304 branded formulations and 20 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Potent inhibitor of serotonin and norepinephrine reuptake transporters (SERT and NET), with weak dopamine reuptake inhibition. Enhances descending inhibitory pain pathways in CNS and PNS, providing antidepressant and analgesic effects. Minimal affinity for muscarinic, histaminergic, and adrenergic receptors.
Avoid in third trimester; risk of neonatal withdrawal and PPHN; use only if benefits outweigh risks in first/second trimester
Excreted in breast milk; use with caution during breastfeeding; monitor infant for sedation and poor feeding
Serotonin syndrome risk.
Contraindicated. Use alternative antibiotic.
Source: DDInter
Risk of serotonin syndrome, hyperthermia, seizures, death
Must wait 14 days between MAOI and duloxetine
Source: Kimi deep-research + Cla
Risk of serotonin syndrome (hyperthermia, rigidity, myoclonus, autonomic instability, mental status changes)
Contraindicated. A washout period of at least 14 days is required between discontinuing an MAOI and starting duloxetine, and at least 5 days between discontinuing duloxetine and starting an MAOI.
CYP2D6 inhibition increases levels of these drugs; QT prolongation risk
Avoid combination
Source: Kimi deep-research + Cla
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Increased plasma concentrations of amitriptyline and its active metabolite nortriptyline, leading to increased risk of anticholinergic effects, sedation, cardiac conduction abnormalities, and seizures.
Avoid concomitant use if possible. If co-administration is necessary, significantly reduce amitriptyline dose (e.g., by 50-75%) and monitor for adverse effects and therapeutic drug levels. Consider alternative antidepressants.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Increased AUC by 2-fold.
Reduce brexpiprazole dose by 50%.
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e, Harrison 22e, Katzung, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19