Sulfasalazine
Contraindicated
Textbook
Exacerbation of inflammatory bowel disease (IBD).
Avoid combining sulfasalazine with traditional NSAIDs.
Source: G&G 14e · p1112
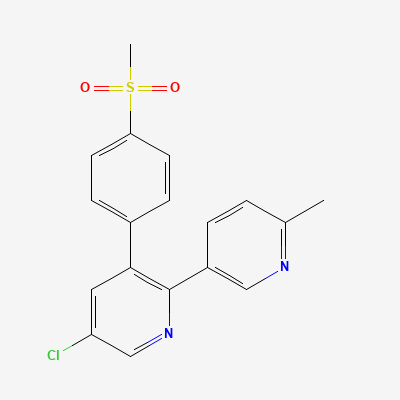
NSAID (selective COX-2 inhibitor / coxib) · Analgesic
Also known as Arcoxia, Nucoxia, Etoshine, Etomark, Brutaflam Etoricoxib
KDIGO 2024 + manufacturer label
1,145 branded formulations and 817 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Selective inhibition of cyclo-oxygenase-2 (COX-2), sparing COX-1-mediated gastric mucosal protection at therapeutic doses
Contraindicated in pregnancy; risk of fetal cardiovascular malformations and premature ductus arteriosus closure
Excretion in breast milk unknown; contraindicated during breastfeeding
Exacerbation of inflammatory bowel disease (IBD).
Avoid combining sulfasalazine with traditional NSAIDs.
Source: G&G 14e · p1112
Increased risk of nephrotoxicity.
Avoid concurrent use.
Source: KDT 7e · p746
Increased aminoglycoside levels and potential toxicity.
Monitor aminoglycoside levels and renal function; adjust dosage as needed.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider alternative analgesics or gastroprotective agents.
Source: KDT 7e
Enhanced CNS toxicity, seizures reported.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Reduced effectiveness of ACE inhibitors. Marked hyperkalemia, potentially leading to cardiac arrhythmia.
Use with caution, especially in the elderly and in patients with hypertension, diabetes mellitus, or ischemic heart disease.
Source: G&G 14e · p836
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19