Ritonavir
Contraindicated
Database
Ergotism: vasospasm, gangrene
Absolute contraindication in HIV patients on PIs.
Source: DDInter
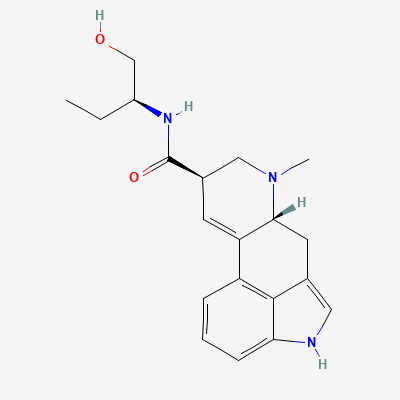
Ergot alkaloid uterotonic agent · Obstetric agent, Postpartum hemorrhage management
Also known as Methylergonovine, Methergine
KDIGO 2024 + manufacturer label
78 branded formulations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Direct agonist at 5-HT2A serotonin and alpha-adrenergic receptors on uterine smooth muscle, causing sustained tetanic uterine contractions. Also has partial agonist/antagonist activity at dopamine D2 receptors. Contracts uterine fundus and mid-zone more than lower segment.
Contraindicated during pregnancy before delivery—causes uterine contractions and fetal distress. Safe for postpartum use.
Excreted in breast milk; may cause GI upset, weakness, and poor feeding in infants. Use lowest effective dose for shortest duration; monitor infant.
Ergotism: vasospasm, gangrene
Absolute contraindication in HIV patients on PIs.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Ergotism
Avoid. Use alternative uterotonic.
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19