Beta Blockers
Moderate
Database
Additive bradycardia + rebound HTN risk on abrupt withdrawal
Taper β-blocker first if stopping moxonidine
Source: Kimi deep-research + Cla
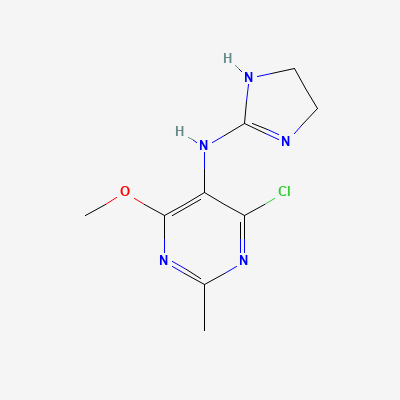
Centrally-acting imidazoline I1 / α2 agonist (antihypertensive) · Antihypertensive
KDIGO 2024 + manufacturer label
Selective agonist at central imidazoline I1 receptors in the rostral ventrolateral medulla (with some α2 activity), reducing sympathetic outflow and lowering blood pressure with less sedation / dry mouth than clonidine.
Avoid (limited data; methyldopa preferred).
Avoid (limited data).
Additive bradycardia + rebound HTN risk on abrupt withdrawal
Taper β-blocker first if stopping moxonidine
Source: Kimi deep-research + Cla
Additive sedation
Avoid alcohol; counsel
Source: Kimi deep-research + Cla
Additive BP lowering
Monitor BP
Source: Kimi deep-research + Cla
Pharmacologic antagonism + additive sedation
Monitor BP; minimise stacking
Source: Kimi deep-research + Cla
Additive bradycardia
Monitor HR
Source: Kimi deep-research + Cla
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e, BNF·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20