Celecoxib
Severe
Textbook-cited
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
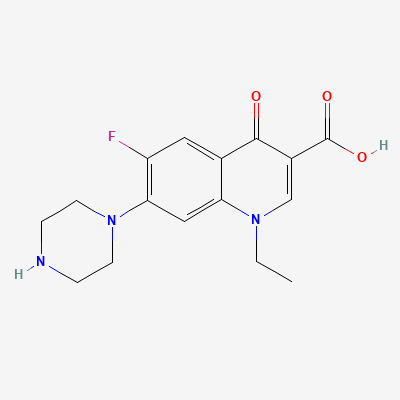
Fluoroquinolone antibiotic · Antibiotic
Also known as Norfloxacin hydrochloride
KDIGO 2024 + manufacturer label
153 branded formulations and 219 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Inhibition of bacterial DNA gyrase (topoisomerase II) and topoisomerase IV, preventing DNA replication, transcription, and repair in susceptible bacteria
Contraindicated in pregnancy - risk of fetal cartilage and joint damage
Excreted in breast milk; contraindicated during breastfeeding
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19