Carbamate Insecticides
Severe
Database
Oxime contraindicated in pure carbamate (worsens weakness)
Identify agent; avoid in pure carbamate
Source: Kimi deep-research + Cla
Cholinesterase reactivator (oxime; organophosphate antidote) · Antidote (for organophosphate poisoning)
KDIGO 2024 + manufacturer label
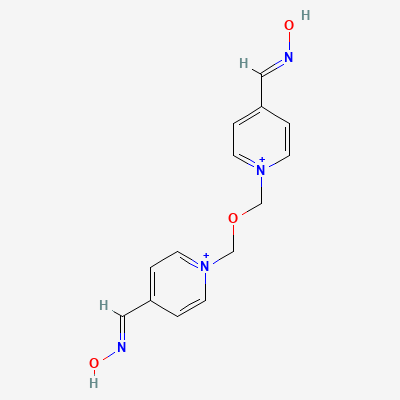
Bisquaternary oxime that reactivates organophosphate-inhibited acetylcholinesterase by removing the phosphoryl group from the enzyme's active site, restoring cholinergic function; effective before 'aging' of the OP-enzyme bond.
Use in life-threatening OP poisoning — benefit outweighs risk.
Limited data; brief use acceptable in emergency.
Oxime contraindicated in pure carbamate (worsens weakness)
Identify agent; avoid in pure carbamate
Source: Kimi deep-research + Cla
Additive hepatic stress
Monitor LFTs with prolonged use
Source: Kimi deep-research + Cla
Duplicate therapy
Do not co-administer
Source: Kimi deep-research + Cla
Altered cholinergic transmission
Caution if anaesthesia needed
Source: Kimi deep-research + Cla
Complementary OP-poisoning treatment
Titrate atropine to dry mucosa; obidoxime per OP confirmation
Source: Kimi deep-research + Cla
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20