Gemfibrozil
Contraindicated
Database
CYP2C8 inhibition → massive repaglinide rise, severe hypoglycaemia
Absolute contraindication — do not co-administer
Source: Kimi deep-research + Cla
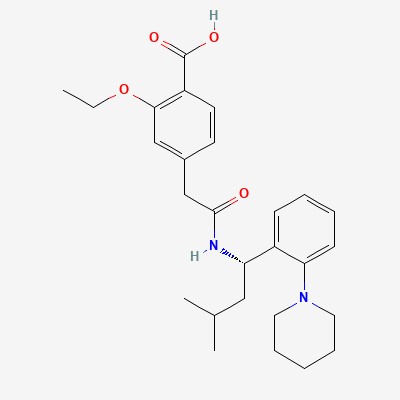
Meglitinide (non-sulfonylurea insulin secretagogue) · Antidiabetic
KDIGO 2024 + manufacturer label
65 branded formulations. Look up specific brands in the Drugs workspace.
Blocks ATP-sensitive potassium (KATP) channels on pancreatic beta-cell membranes, causing membrane depolarization, calcium influx, and insulin secretion. Rapid onset and short duration—stimulates prandial insulin secretion. Closes KATP channels at a different binding site than sulfonylureas.
Not recommended in pregnancy—insulin is preferred for glycemic control. Animal data show no teratogenicity at therapeutic doses.
Excretion in breast milk unknown; not recommended during breastfeeding.
CYP2C8 inhibition → massive repaglinide rise, severe hypoglycaemia
Absolute contraindication — do not co-administer
Source: Kimi deep-research + Cla
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: antagonism.
Source: DDInter
Drug interactions with repaglinide, potentially increasing its concentration and effect.
Monitor for altered effects of repaglinide if coadministration is necessary.
Source: DDInter
Potentiation of repaglinide's action, increasing risk of hypoglycemia.
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
.
Source: DDInter
Clinical effect not specified
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19