Cisapride
Contraindicated
Database
Possible rise in plasma levels of cisapride.
Exercise caution.
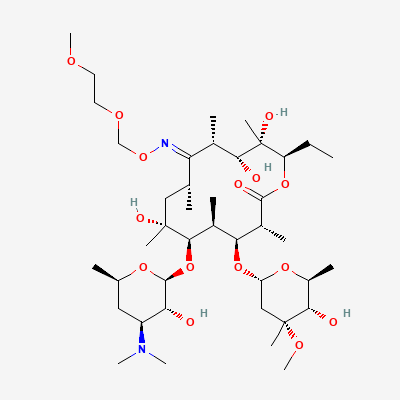
Semisynthetic 14-membered macrolide antibiotic · Antibacterial
KDIGO 2024 + manufacturer label
Binds the bacterial 50S ribosomal subunit, inhibiting protein synthesis; bacteriostatic against Gram-positive cocci, atypicals (Mycoplasma, Chlamydia, Legionella) and some Gram-negatives.
Use only if clearly needed; macrolide class generally acceptable.
Small amounts in milk; generally compatible.
Possible rise in plasma levels of cisapride.
Exercise caution.
Increased plasma concentrations of ergotamine, leading to ergotism (vasospasm, ischemia of extremities and other tissues).
Concomitant use is contraindicated due to the risk of severe and potentially life-threatening vasospasm. Avoid completely.
Increased pimozide levels, leading to QT prolongation and potentially fatal ventricular arrhythmias (e.g., Torsades de Pointes).
Concomitant use is contraindicated. Avoid completely.
Reduced ergot metabolism
Contraindicated
Source: Kimi deep-research + Cla
Colchicine toxicity (gastrointestinal symptoms, myelosuppression, rhabdomyolysis, neuropathy).
Avoid concomitant use. If unavoidable, significantly reduce colchicine dose and monitor closely for toxicity.
Possible rise in plasma levels of terfenadine.
Exercise caution.
Source: KDT 7e · p754
Increased risk of ventricular arrhythmias, including Torsades de Pointes.
Avoid concomitant use in patients with risk factors for QT prolongation (e.g., hypokalemia, bradycardia, pre-existing heart disease). If co-administration is necessary, monitor ECG and electrolytes. Consider alternative antibiotics.
Increased bromocriptine levels, leading to increased risk of adverse effects (e.g., nausea, vomiting, hypotension, hallucinations).
Monitor for increased adverse effects of bromocriptine. Consider reducing bromocriptine dose.
Increased carbamazepine levels, leading to increased risk of toxicity (e.g., dizziness, ataxia, diplopia, nausea, vomiting).
Monitor carbamazepine levels and clinical signs of toxicity. Reduce carbamazepine dose if necessary.
Increased risk of ciclosporin toxicity (nephrotoxicity, neurotoxicity, hepatotoxicity).
Monitor ciclosporin trough levels closely. Adjust ciclosporin dose as needed.
Increased cyclosporine levels, leading to increased risk of nephrotoxicity and other adverse effects.
Monitor cyclosporine levels closely. Reduce cyclosporine dose as needed. Monitor renal function.
Increased digoxin levels and potential for digoxin toxicity (nausea, vomiting, arrhythmias).
Monitor digoxin levels and clinical signs of toxicity. Reduce digoxin dose if necessary. Consider alternative antibiotics if possible.
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20