Thiopental
Contraindicated
Textbook
Chemical reaction occurs when mixed.
Should not be mixed in the same syringe.
Source: KDT 7e · p347-359
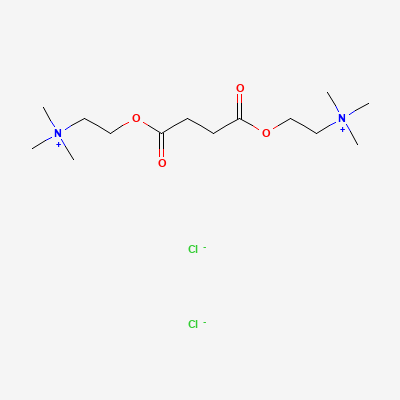
Depolarising neuromuscular blocker (ultra-short) · Skeletal Muscle Relaxant; Adjunct to Anesthesia
Also known as Suxamethonium, Suxamethonium Chloride, Anectine, Quelicin
KDIGO 2024 + manufacturer label
6 branded formulations. Look up specific brands in the Drugs workspace.
Binds nicotinic ACh receptors at the motor end-plate causing persistent depolarisation (phase I block) → transient fasciculations then flaccid paralysis; hydrolysed by plasma pseudocholinesterase.
Acceptable for obstetric anaesthesia (minimal placental transfer).
Not relevant (single peri-procedural use; rapidly hydrolysed).
Chemical reaction occurs when mixed.
Should not be mixed in the same syringe.
Source: KDT 7e · p347-359
MH-trigger synergy
Avoid in MH-susceptible; have dantrolene available
Source: Kimi deep-research + Cla
Prolonged paralysis.
Not explicitly stated
Source: KDT 7e
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Neostigmine is not effective against the skeletal muscle paralysis caused by succinylcholine; instead, it will enhance depolarization and the resultant blockade, potentially worsening paralysis.
Avoid combination or use with extreme caution. Neostigmine should not be used to reverse succinylcholine-induced paralysis.
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20