Bisphosphonates
Moderate
Database
Reduced absorption
Separate widely
Source: Kimi deep-research + Cla
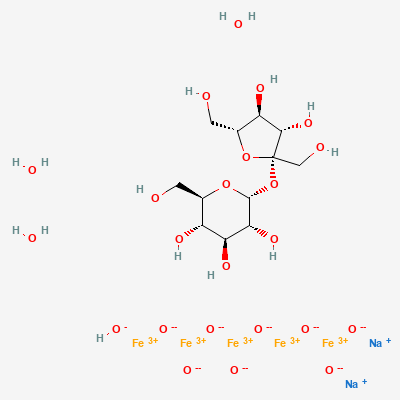
Iron-based phosphate binder (non-calcium) · Phosphate-binding agent
KDIGO 2024 + manufacturer label
Polynuclear iron(III) oxyhydroxide stabilised on sucrose/starch — binds dietary phosphate in the gut by ligand exchange forming insoluble iron-phosphate; lowers serum phosphate in dialysis-dependent CKD with negligible iron absorption.
Limited data; phosphate control may be needed.
Minimal absorption — likely compatible.
Reduced absorption
Separate widely
Source: Kimi deep-research + Cla
Iron-tetracycline chelation
Separate dosing
Source: Kimi deep-research + Cla
Iron-quinolone chelation
Separate by ≥2 h
Source: Kimi deep-research + Cla
Reduced thyroxine absorption
Separate by ≥4 h; monitor TSH
Source: Kimi deep-research + Cla
Combined phosphate binding (sometimes intended)
Adjust per phosphate response
Source: Kimi deep-research + Cla
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20