Dofetilide
Severe
Database
Clinical effect not specified
Source: DDInter
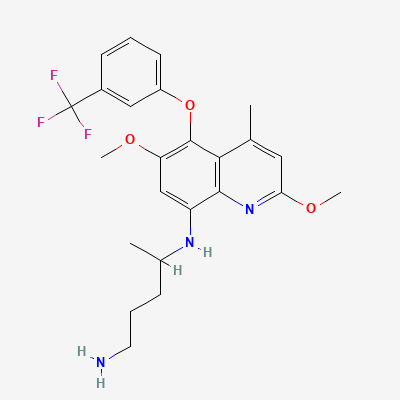
8-Aminoquinoline antimalarial (radical cure) · Antimalarial
KDIGO 2024 + manufacturer label
8-aminoquinoline with active metabolites that produce reactive oxygen species lethal to Plasmodium hypnozoites in the liver — provides radical cure of P. vivax / P. ovale relapsing malaria; activity against hepatic and erythrocytic stages.
Contraindicated (limited data; theoretical fetal haemolysis if fetus G6PD-deficient).
Avoid breastfeeding G6PD-deficient infants; otherwise weigh risk.
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Additive methaemoglobinaemia
Avoid combination
Source: Kimi deep-research + Cla
Duplicate therapy + additive haemolysis
Do not co-administer
Source: Kimi deep-research + Cla
Tafenoquine inhibits OCT2 / MATE
Monitor metformin levels / clinical effect
Source: Kimi deep-research + Cla
6 additional low-confidence interactions hidden — those rows lack a documented mechanism or management plan in our sources.
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20