Adrenaline
Severe
Textbook
Marked rise in BP.
Adrenaline should not be given to patients receiving β blockers.
Source: KDT 7e · p133
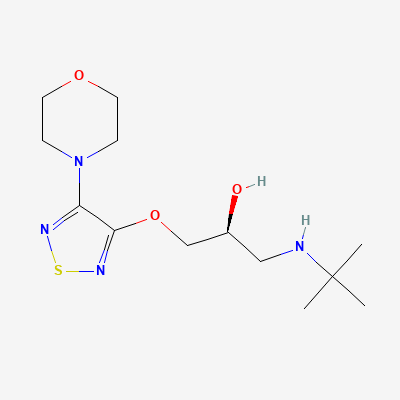
Non-selective beta-adrenergic receptor antagonist (beta-blocker) · Antihypertensive
Also known as Timolol maleate, Timoptic, Betimol
KDIGO 2024 + manufacturer label
82 branded formulations and 65 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Non-selective competitive antagonism of beta-1 and beta-2 adrenergic receptors; reduces heart rate, myocardial contractility, and aqueous humor production
Small amounts cross placenta; may cause fetal bradycardia, hypoglycemia. Use only if benefit outweighs risk—prefer cardioselective beta-blockers in pregnancy.
Excreted in breast milk in small amounts; plasma levels in nursing infants estimated at 1-2% of maternal level. Generally considered compatible but monitor infant for bradycardia and hypoglycemia.
Marked rise in BP.
Adrenaline should not be given to patients receiving β blockers.
Source: KDT 7e · p133
Hyperkalaemia more likely.
Source: KDT 7e
Severe bradycardia.
Extreme caution advised if amiodarone is co-administered with sofosbuvir and a beta blocker.
Source: Harrison 22e · unknown
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Beta-blocker masks clonidine withdrawal rebound hypertension; abrupt discontinuation of either can cause hypertensive crisis.
Withdraw beta-blocker first, then taper clonidine over several days. Monitor BP closely.
Source: Kimi deep-research + Cla
Increased propensity for AV block, severe bradycardia, and decreased left ventricular function.
Avoid concurrent administration. The concurrent administration of diltiazem with a beta blocker is contraindicated.
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19