Furosemide
Severe
Textbook-cited
Ototoxicity (hearing loss) and nephrotoxicity.
Avoid concurrent use; if unavoidable, monitor renal function and audiometry
Source: KDT 7e · p949
Aminoglycoside antibiotic · Antibiotic
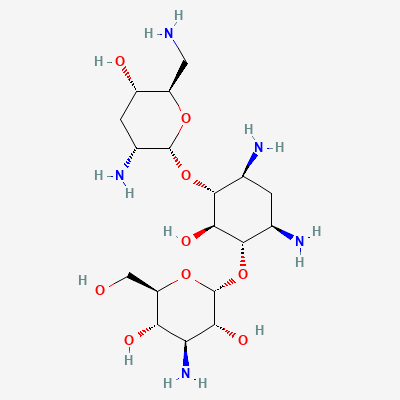
Also known as Tobramycin Sulfate, Nebcin, Tobi, Bethkis, Kitabis Pak, Tobrex
KDIGO 2024 + manufacturer label
193 branded formulations and 19 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Binds irreversibly to 30S ribosomal subunit, inhibiting bacterial protein synthesis. Bactericidal against aerobic Gram-negative bacilli including Pseudomonas aeruginosa, Enterobacterales, and Acinetobacter. Poor activity against anaerobes and most Gram-positive organisms (except Staphylococcus aureus in combination).
Avoid in pregnancy unless no alternative; ototoxicity risk to fetus; Category D
Excreted in breast milk in small amounts; compatible with breastfeeding per AAP; monitor infant for diarrhea and thrush
Ototoxicity (hearing loss) and nephrotoxicity.
Avoid concurrent use; if unavoidable, monitor renal function and audiometry
Source: KDT 7e · p949
Additive nephrotoxicity
Avoid if possible; monitor renal function closely
Source: Kimi deep-research + Cla
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Increased risk of severe nephrotoxicity and ototoxicity (hearing loss, tinnitus). Both drugs are independently nephrotoxic and ototoxic.
Avoid concomitant use if possible. If co-administration is unavoidable, monitor renal function and auditory function very closely. Adjust tobramycin dose based on renal function. Consider alternative antibiotics.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19