Cilostazole
Contraindicated
Textbook
Increased plasma levels and toxicity of cilostazole.
Should not be administered along with inhibitors of CYP3A4.
Source: KDT 7e · p555
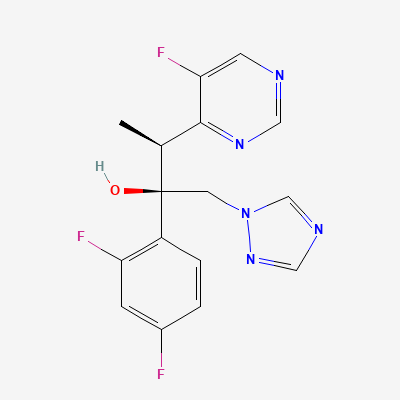
Triazole antifungal agent (broad-spectrum) · Antifungal
Also known as Vfend, Voriconazole IV, Voriconazole oral
KDIGO 2024 + manufacturer label
77 branded formulations. Look up specific brands in the Drugs workspace.
Inhibits fungal cytochrome P450-dependent enzyme lanosterol 14α-demethylase, blocking conversion of lanosterol to ergosterol (essential fungal cell membrane component). Disrupts cell membrane synthesis, causing cell death. Broad spectrum including Aspergillus, Candida (including fluconazole-resistant), Fusarium, Scedosporium.
Contraindicated in pregnancy—teratogenic in animals (cleft palate, skeletal defects). Effective contraception required during and for 1 month after treatment.
Excreted in breast milk; avoid during breastfeeding.
Increased plasma levels and toxicity of cilostazole.
Should not be administered along with inhibitors of CYP3A4.
Source: KDT 7e · p555
Markedly reduces voriconazole levels; rifampicin reduces voriconazole Cmax by ~93%.
Absolutely contraindicated. Use alternative antifungal if these drugs are essential.
Source: Kimi deep-research + Cla
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Increase amiodarone levels.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19