Gatifloxacin
Severe
Database
Drug interaction classified as: antagonism
Source: DDInter
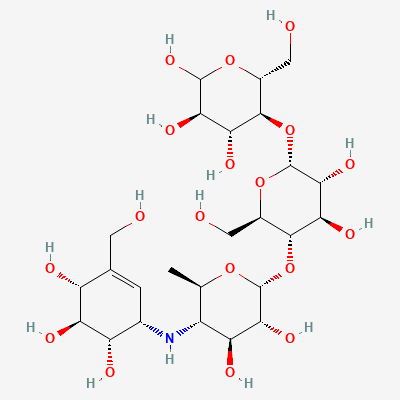
α-Glucosidase inhibitor (antidiabetic) · Antidiabetic
KDIGO 2024 + manufacturer label
Reversibly inhibits intestinal brush-border α-glucosidases (sucrase, maltase, glucoamylase), delaying carbohydrate digestion and absorption; flattens postprandial glucose rise without intrinsic hypoglycaemia risk.
Generally not recommended (insulin preferred in pregnancy).
Limited data; minimal systemic absorption.
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Reduced efficacy of acarbose in controlling postprandial glucose levels, as pancreatin's amylase activity may counteract acarbose's mechanism of action.
Monitor blood glucose levels closely. If concurrent use is necessary, consider adjusting the dose of acarbose or pancreatin, or administering them at different times. The clinical significance is generally considered low unless very high doses of pancreatin are used.
5 additional low-confidence interactions hidden — those rows lack a documented mechanism or management plan in our sources.
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, BNF·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20