Agents With Antimuscarinic Activity
Contraindicated
Textbook
Their antimuscarinic action is likely to intensify the toxicity of atropine poisoning.
Agents with antimuscarinic activity should not be used in atropine poisoning.
Source: G&G 14e · p218
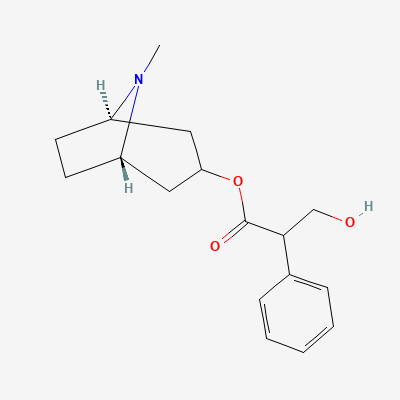
Antimuscarinic agent (non-selective muscarinic receptor antagonist) · Antidysrhythmic, Mydriatic, Antidote, Antispasmodic, Pre-anesthetic
Also known as Atropine Sulfate, Atropisol, Isopto Atropine
KDIGO 2024 + manufacturer label
59 branded formulations and 10 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Competitive antagonist of acetylcholine at all muscarinic receptor subtypes (M1-M5), blocking parasympathetic effects on smooth muscle, cardiac muscle, exocrine glands, and the eye. Increases heart rate, reduces secretions, dilates pupils, relaxes smooth muscle.
Crosses placenta; may cause fetal tachycardia. Use only if clearly needed. Safe for short-term use.
Excreted in breast milk in small amounts; may reduce milk production. Use lowest effective dose; monitor infant for anticholinergic effects.
Their antimuscarinic action is likely to intensify the toxicity of atropine poisoning.
Agents with antimuscarinic activity should not be used in atropine poisoning.
Source: G&G 14e · p218
Their antimuscarinic action is likely to intensify the toxicity of atropine poisoning.
Phenothiazines should not be used in atropine poisoning.
Source: G&G 14e · p218
Atropine effectively antagonizes muscarinic symptoms of anti-ChE agent poisoning, such as increased tracheobronchial and salivary secretion, bronchoconstriction, and bradycardia. It can also control muscarinic cardiovascular and GI side effects of anti-ChE agents.
In organophosphate poisoning, atropine should be given in doses sufficient to cross the blood-brain barrier: an initial injection of 2 to 4 mg intravenously (or intramuscularly), followed by 2 mg every 5 to 10 minutes until muscarinic symptoms disappear, reappear, or signs of atropine toxicity occur. However, anticholinergic drugs like atropine can mask many side effects of an excessive dose of an anti-ChE agent.
Source: G&G 14e · p228, p230, p232
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
If marked excitement is present in atropine poisoning and more specific treatment is not available, benzodiazepines can provide sedation and control convulsions.
A benzodiazepine is the most suitable agent for sedation and control of convulsions.
Source: G&G 14e · p218
Increased anticholinergic side effects.
Source: KDT 7e · p121
If marked excitement is present in atropine poisoning and more specific treatment is not available, benzodiazepines can provide sedation and control convulsions.
A benzodiazepine is the most suitable agent for sedation and control of convulsions.
Source: G&G 14e · p218
If marked excitement is present in atropine poisoning and more specific treatment is not available, benzodiazepines can provide sedation and control convulsions.
A benzodiazepine is the most suitable agent for sedation and control of convulsions.
Source: G&G 14e · p218
If marked excitement is present in atropine poisoning and more specific treatment is not available, benzodiazepines can provide sedation and control convulsions.
A benzodiazepine is the most suitable agent for sedation and control of convulsions.
Source: G&G 14e · p218
If marked excitement is present in atropine poisoning and more specific treatment is not available, benzodiazepines can provide sedation and control convulsions.
A benzodiazepine is the most suitable agent for sedation and control of convulsions.
Source: G&G 14e · p218
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19