Carbamazepine
Severe
Database
Drug interaction classified as: metabolism
Source: DDInter
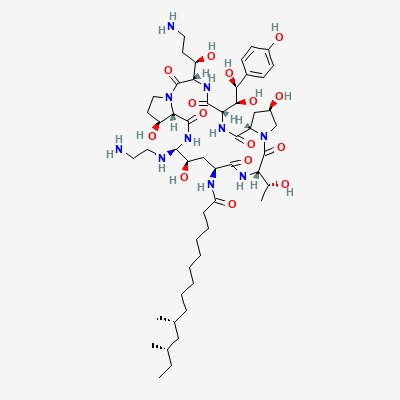
Echinocandin antifungal · Antifungal
Also known as Caspofungin acetate, Cancidas, Casporex
KDIGO 2024 + manufacturer label
51 branded formulations. Look up specific brands in the Drugs workspace.
Non-competitive inhibition of 1,3-beta-D-glucan synthase, disrupting fungal cell-wall synthesis → osmotic lysis; fungicidal against Candida, fungistatic against Aspergillus. No human cell-wall target → favourable safety.
Use only if benefit outweighs risk — animal embryotoxicity; limited human data
Unknown excretion; caution
Drug interaction classified as: metabolism
Source: DDInter
Increased caspofungin AUC + raised transaminases
Use only if benefit outweighs risk; monitor LFTs
Source: Kimi deep-research + Cla
Drug interaction classified as: metabolism.
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19