Aminophylline
Contraindicated
Textbook
Should not be mixed in the same infusion bottle/syringe.
Do not mix.
Source: KDT 7e · p227
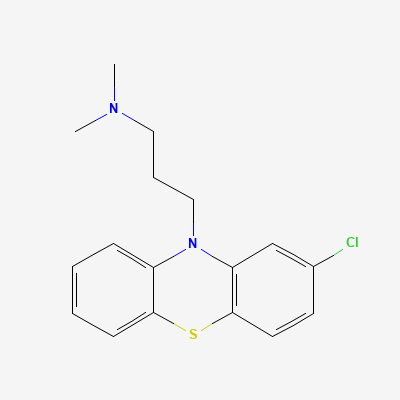
Typical (first-generation) phenothiazine antipsychotic · Antipsychotic
Also known as Chlorpromazine Hydrochloride, CPZ, Thorazine, Largactil
KDIGO 2024 + manufacturer label
67 branded formulations and 59 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Non-selective dopamine D2 receptor antagonism (mesolimbic pathway = antipsychotic effect; nigrostriatal = EPS; tuberoinfundibular = hyperprolactinemia). Also blocks α1-adrenergic, muscarinic, and histamine H1 receptors.
Crosses placenta; may cause extrapyramidal symptoms and withdrawal in neonates if used near term. Use only if benefit outweighs risk.
Excreted in breast milk; may cause drowsiness and EPS in infant. Use lowest effective dose; consider alternative antipsychotic.
Should not be mixed in the same infusion bottle/syringe.
Do not mix.
Source: KDT 7e · p227
Enhanced sedation and respiratory depression.
Avoid concurrent use
Source: KDT 7e · p950
Excessive sedation, respiratory depression, motor impairment.
Avoid concurrent use
Source: KDT 7e · p950
Excessive sedation and respiratory depression; potentially fatal.
Avoid concurrent use
Source: KDT 7e · p950
Severe sedation and respiratory depression
Avoid concurrent use
Source: KDT 7e · p950
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19