Gatifloxacin
Severe
Database
Clinical effect not specified
Source: DDInter
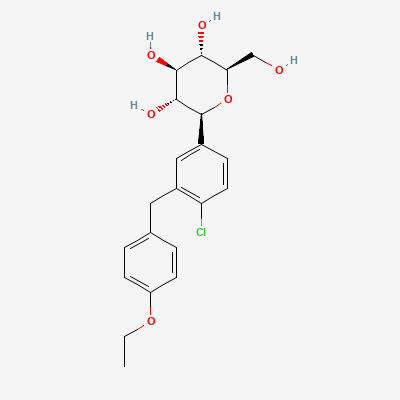
Sodium-glucose cotransporter 2 (SGLT2) inhibitor (gliflozin) · Antidiabetic
Also known as Dapagliflozin propanediol, Forxiga, Farxiga, Oxra
KDIGO 2024 + manufacturer label
263 branded formulations and 39 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Selective inhibition of SGLT2 in proximal renal tubule, reducing renal glucose reabsorption and promoting urinary glucose excretion (glycosuria). This results in insulin-independent glucose lowering, osmotic diuresis, natriuresis, and modest weight loss. Cardiac benefits likely mediated by improved cardiac energetics, reduced preload/afterload, and anti-fibrotic effects.
Avoid in second and third trimesters; animal studies show renal developmental toxicity; limited data in first trimester
Excreted in breast milk; avoid during breastfeeding
Clinical effect not specified
Source: DDInter
Increased risk of hypotension and potential for acute kidney injury, especially in patients with pre-existing renal impairment or volume depletion.
Monitor blood pressure and renal function closely, especially at initiation of therapy or dose changes. Ensure adequate hydration. Consider dose adjustment of either agent if hypotension or renal dysfunction occurs.
Increased risk of hypotension and potential for acute kidney injury, especially in patients with pre-existing renal impairment or volume depletion.
Monitor blood pressure and renal function closely, especially at initiation of therapy or dose changes. Ensure adequate hydration. Consider dose adjustment of either agent if hypotension or renal dysfunction occurs.
Excessive diuresis, dehydration, hypotension, AKI
Monitor volume status. Reduce furosemide dose.
Source: DDInter
SGLT2 inhibition reduces renal lithium clearance; can cause lithium toxicity
Monitor lithium levels closely; avoid if possible
Source: Kimi deep-research + Cla
Additive volume depletion and hypotension risk; may precipitate AKI
Monitor volume status, renal function, and BP; consider reducing diuretic dose
Source: Kimi deep-research + Cla
NSAIDs can impair renal function and, in combination with dapagliflozin's diuretic effect, may increase the risk of acute kidney injury, especially in volume-depleted patients or those with pre-existing renal impairment.
Monitor renal function closely, especially in patients at higher risk. Ensure adequate hydration. Avoid concomitant use in patients with significant renal impairment or volume depletion if possible.
Reduced SGLT2i levels
Monitor glucose. May need dose adjustment.
Source: DDInter
Hypotension, dehydration
Monitor volume status and electrolytes.
Source: DDInter
Increased risk of hypoglycemia.
When dapagliflozin is added to sulfonylurea therapy, a lower dose of the sulfonylurea may be required to minimize the risk of hypoglycemia. Monitor blood glucose levels closely and adjust sulfonylurea dose as needed.
Increased risk of dehydration, hypovolemia, and hypotension, especially in elderly patients or those with impaired renal function.
Monitor for signs and symptoms of dehydration and hypotension. Consider reducing the dose of the thiazide diuretic or dapagliflozin, or temporarily discontinuing dapagliflozin during periods of acute illness or dehydration.
1 additional low-confidence interaction hidden — those rows lack a documented mechanism or management plan in our sources.
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19