Alcohol
Contraindicated
Database
Additive CNS/respiratory depression
Avoid; major contributor to historical deaths
Source: Kimi deep-research + Cla
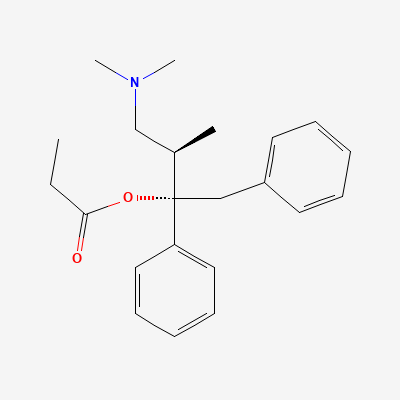
Opioid analgesic (weak mu-agonist; largely withdrawn) · analgesic
KDIGO 2024 + manufacturer label
Weak mu-opioid receptor agonist; the metabolite norpropoxyphene is cardiotoxic (sodium-channel blockade → QRS/QT prolongation, arrhythmia), which underlies its withdrawal from many markets.
Avoid; neonatal withdrawal/respiratory depression.
Small amounts in milk; avoid (safer alternatives).
Additive CNS/respiratory depression
Avoid; major contributor to historical deaths
Source: Kimi deep-research + Cla
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy, metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy, metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy, metabolism
Source: DDInter
Drug interaction classified as: synergy, metabolism
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20