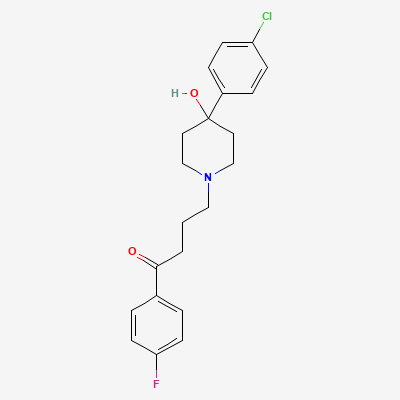
Domperidone
Contraindicated
Database
Increased risk of QT prolongation and Torsades de Pointes (TdP)
Concomitant use is contraindicated. Avoid co-administration.
First-generation (typical) antipsychotic (butyrophenone) · Antipsychotic
Also known as Haloperidol decanoate, Haldol, Serenace
KDIGO 2024 + manufacturer label
248 branded formulations and 18 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Potent antagonist at dopamine D2 receptors in mesolimbic pathway (antipsychotic effect), nigrostriatal pathway (extrapyramidal side effects), and tuberoinfundibular pathway (hyperprolactinemia). Also has antagonist activity at alpha-1 adrenergic receptors and weak anticholinergic effects.
Use only if benefits outweigh risks; neonatal EPS and withdrawal reported; third trimester exposure risk
Excreted in breast milk; small amounts; monitor infant for sedation and EPS
Increased risk of QT prolongation and Torsades de Pointes (TdP)
Concomitant use is contraindicated. Avoid co-administration.
Additive QT prolongation; high risk of torsades de pointes
Avoid combination; monitor QTc if unavoidable
Source: Kimi deep-research + Cla
Excessive sedation, respiratory depression, motor impairment.
Avoid concurrent use
Source: KDT 7e · p950
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19