Aromatase Inhibitors
Moderate
Database
Possible interference with oestrogen suppression
Avoid in patients on AIs
Source: Kimi deep-research + Cla
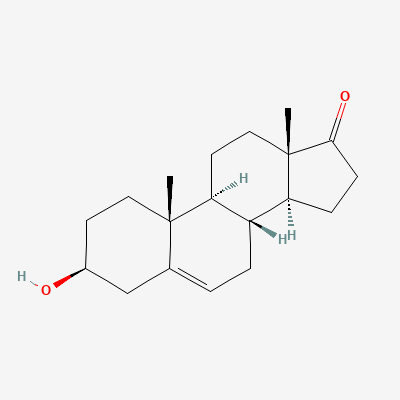
Endogenous adrenal steroid (DHEA) — vaginal preparation · Gynecological Agent
KDIGO 2024 + manufacturer label
Dehydroepiandrosterone (DHEA) is converted intracellularly to androgens and oestrogens via vaginal cell steroidogenesis (intracrinology), restoring local hormonal environment for vulvovaginal atrophy of menopause — minimal systemic hormonal exposure.
Not applicable (postmenopausal indication).
Not applicable.
Possible interference with oestrogen suppression
Avoid in patients on AIs
Source: Kimi deep-research + Cla
Possible duplicate hormonal effects
Avoid concomitant systemic HRT for the same indication
Source: Kimi deep-research + Cla
Minor INR changes possible
Monitor INR if combined
Source: Kimi deep-research + Cla
Local intracrinology; minimal systemic CYP effect
No action
Source: Kimi deep-research + Cla
DHEA may modestly affect insulin sensitivity
Routine monitoring
Source: Kimi deep-research + Cla
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20