Sacubitril Valsartan
Contraindicated
Textbook
Increased risk of angioedema.
Do not use in conjunction with ACEIs.
Source: G&G 14e · p602
ACE Inhibitor · Antihypertensive
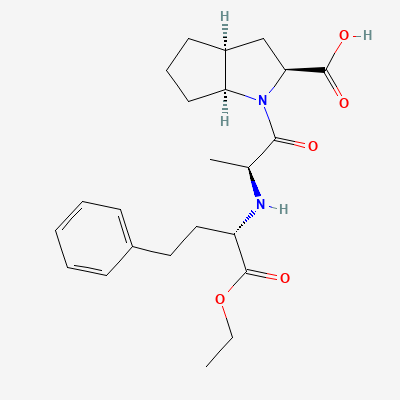
Also known as Ramiprilat, Cardace, Ramistar, Zaram, Acovil
KDIGO 2024 + manufacturer label
400 branded formulations and 107 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Ramipril is a prodrug that is hydrolyzed in the liver to its active metabolite, ramiprilat. Ramiprilat competitively inhibits angiotensin-converting enzyme (ACE), thereby preventing the conversion of angiotensin I to the potent vasoconstrictor angiotensin II. This inhibition leads to decreased systemic vascular resistance, reduced aldosterone secretion, and increased bradykinin levels, resulting in vasodilation, natriuresis, and reduced cardiac remodeling.
Category D — fetal renal injury, oligohydramnios
Excreted into breast milk. Not recommended during breastfeeding due to potential adverse effects on the infant (e.g., hypotension, hyperkalemia).
Increased risk of angioedema.
Do not use in conjunction with ACEIs.
Source: G&G 14e · p602
Increased risk of hypotension, hyperkalemia, and renal impairment (including acute renal failure) compared to monotherapy, with no proven additional benefit.
Contraindicated. Avoid concomitant use, especially in patients with diabetes or renal impairment.
Fatal angioedema
Wait 36 hours after stopping ACEi before starting ARNI.
Significantly increased risk of angioedema, a potentially life-threatening swelling of the face, lips, tongue, and throat.
Contraindicated. A washout period of at least 36 hours is required between discontinuing ramipril and initiating sacubitril/valsartan, and vice versa.
Increased risk and severity of renal impairment and nephrotoxicity.
Not explicitly stated, but implies careful monitoring of renal function and cautious co-administration.
Source: G&G 14e
Greater incidence of acute kidney injury (AKI) and adverse cardiac events.
The combination of these two classes should be avoided.
Source: Harrison 22e · p2396
Increased worsening of renal function, hypotension, syncope, and hyperkalemia without increased efficacy.
Not recommended for the treatment of hypertension. Previous studies indicate more harm than benefit.
Source: G&G 14e
Increased worsening of renal function, hypotension, syncope, and hyperkalemia without increased efficacy.
Not recommended for the treatment of hypertension. Previous studies indicate more harm than benefit.
Source: G&G 14e
Increased risk of angioedema.
Avoid combination.
Source: G&G 14e · p600
Increased worsening of renal function, hypotension, syncope, and hyperkalemia without increased efficacy.
Not recommended for the treatment of hypertension. Previous studies indicate more harm than benefit.
Source: G&G 14e
Increased worsening of renal function, hypotension, syncope, and hyperkalemia without increased efficacy.
Not recommended for the treatment of hypertension. Previous studies indicate more harm than benefit.
Source: G&G 14e
Increased worsening of renal function, hypotension, syncope, and hyperkalemia without increased efficacy.
Not recommended for the treatment of hypertension. Previous studies indicate more harm than benefit.
Source: G&G 14e
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-17 · House clinical team·Cockpit curated: 2026-05-16