Acetazolamide
Severe
Database
Severe metabolic acidosis, nephrolithiasis.
Avoid combination.
Source: DDInter
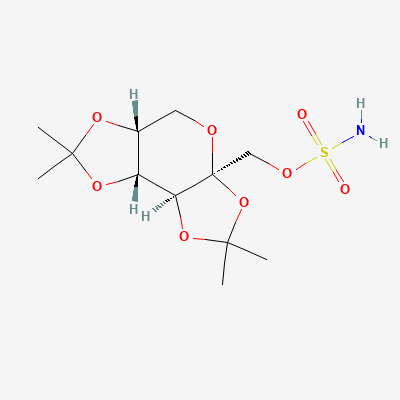
Sulfamate-substituted monosaccharide antiepileptic · Antiepileptic
KDIGO 2024 + manufacturer label
135 branded formulations. Look up specific brands in the Drugs workspace.
Multiple mechanisms: blocks voltage-gated sodium channels, enhances GABA-A receptor activity, inhibits AMPA/kainate glutamate receptors, and weakly inhibits carbonic anhydrase isoenzymes II and IV
Teratogenic—dose-dependent risk of oral clefts (cleft lip/palate) and low birth weight. Pregnancy registry data show 1.2-1.4% risk of oral clefts vs 0.4% baseline. Minimum effective dose advised if treatment essential.
Excreted in breast milk (milk:plasma ratio ~0.6-1.1); infant exposure ~10-20% of maternal dose. Sedation and diarrhea reported in infants. Use with caution during breastfeeding.
Severe metabolic acidosis, nephrolithiasis.
Avoid combination.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19