Amprenavir
Severe
Database
Drug interaction classified as: metabolism
Source: DDInter
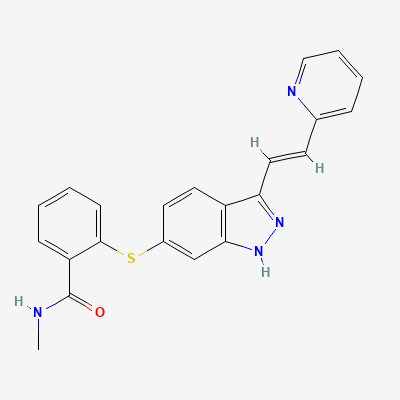
Selective VEGFR tyrosine kinase inhibitor (antineoplastic) · Antineoplastic agent
Also known as Inlyta
KDIGO 2024 + manufacturer label
Selective ATP-competitive inhibitor of VEGFR-1/2/3 tyrosine kinases, blocking VEGF-mediated tumour angiogenesis; less off-target activity (PDGFR, c-KIT) than first-gen TKIs.
Can cause fetal harm — avoid; effective contraception during and 1 week after.
Avoid breastfeeding during and 2 weeks after therapy.
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20