Adalimumab
Severe
Database
Drug interaction classified as: synergy
Source: DDInter
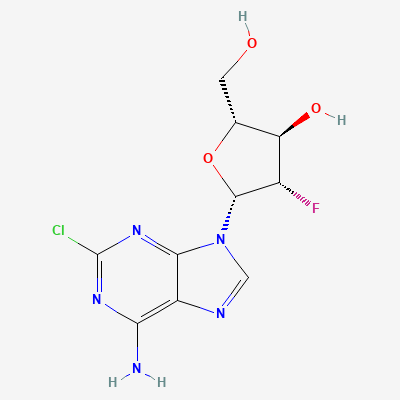
Antineoplastic purine nucleoside analogue · Anticancer
KDIGO 2024 + manufacturer label
Intracellularly phosphorylated to clofarabine triphosphate, which inhibits DNA polymerase and ribonucleotide reductase and disrupts mitochondrial membrane integrity — terminating DNA synthesis and inducing apoptosis in leukaemic blasts.
Can cause fetal harm — avoid; effective contraception required.
Contraindicated during therapy.
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Additive hepatotoxicity (VOD risk)
Avoid; monitor LFTs closely
Source: Kimi deep-research + Cla
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e, BNF·Verified: 2026-05-20 · House clinical team·Cockpit curated: 2026-05-20