Furosemide
Severe
Textbook-cited
Digoxin toxicity (arrhythmias, nausea, visual disturbances).
Co-prescribe potassium-sparing diuretic or potassium supplements
Source: KDT 7e · p949
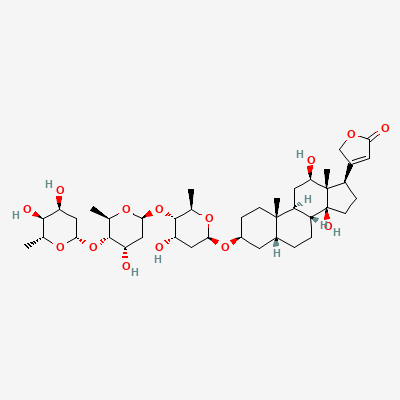
Cardiac Glycoside · Cardiac
Also known as Lanoxin, Digitalis
KDIGO 2024 + manufacturer label
20 branded formulations. Look up specific brands in the Drugs workspace.
Digoxin inhibits the Na+/K+-ATPase pump in myocardial cells, leading to increased intracellular sodium. This in turn reduces the activity of the Na+/Ca++ exchanger, increasing intracellular calcium concentration. The elevated calcium enhances myocardial contractility (positive inotropy) and prolongs the effective refractory period of the AV node, thus slowing ventricular rate in atrial fibrillation. It also increases vagal tone.
Category C — used for fetal SVT; otherwise crosses placenta freely
Digoxin is excreted into breast milk in small amounts. Generally considered compatible with breastfeeding, but monitor the infant for signs of toxicity (e.g., bradycardia, vomiting).
Digoxin toxicity (arrhythmias, nausea, visual disturbances).
Co-prescribe potassium-sparing diuretic or potassium supplements
Source: KDT 7e · p949
Digoxin toxicity (arrhythmias, nausea, visual disturbances).
Co-prescribe potassium-sparing diuretic or potassium supplements
Source: KDT 7e · p949
Digoxin toxicity (arrhythmias, nausea, visual disturbances).
Co-prescribe potassium-sparing diuretic or potassium supplements
Source: KDT 7e · p949
can induce arrhythmias
not specified
Source: KDT 7e · p517
Increased plasma levels of digoxin.
Source: Harrison 22e · p1742
Reduced oral bioavailability of digoxin.
Source: KDT 7e · p15
Drug interaction classified as: synergy.
Source: DDInter
P-gp inhibition → doubled digoxin levels/toxicity
Halve digoxin dose; monitor levels
Source: Kimi deep-research + Cla
Amphotericin hypokalaemia potentiates digoxin toxicity
Monitor K+ and digoxin; replete potassium
Source: Kimi deep-research + Cla
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-16 · House clinical team·Cockpit curated: 2026-05-16