Amitriptyline
Severe
Database
Drug interaction classified as: synergy.
Source: DDInter
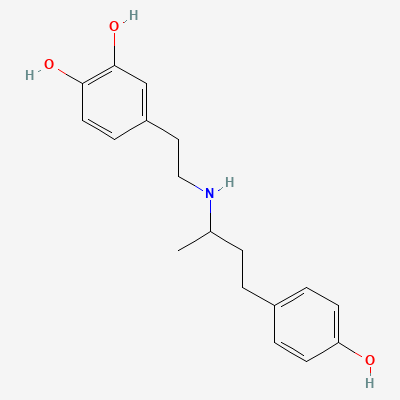
Beta-1 selective inotrope (synthetic catecholamine) · Cardiac stimulant
Also known as Dobutamine hydrochloride
KDIGO 2024 + manufacturer label
32 branded formulations. Look up specific brands in the Drugs workspace.
Predominant beta-1 adrenergic agonism increasing myocardial contractility and stroke volume with relatively modest chronotropy; mild beta-2 vasodilation and alpha effects (racemate) → improved cardiac output, usually reduced systemic vascular resistance.
Use only for serious maternal haemodynamic indication — limited data
Acute critical-care use; minimal relevance (very short t½) — caution
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Clinical effect not specified
Source: DDInter
Antagonise inotropy; unopposed alpha → severe hypertension
Avoid; if needed titrate carefully under monitoring
Source: Kimi deep-research + Cla
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
.
Source: DDInter
Potentiated pressor/arrhythmic response
Avoid; great caution
Source: Kimi deep-research + Cla
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19