Amprenavir
Severe
Database
Drug interaction classified as: metabolism
Source: DDInter
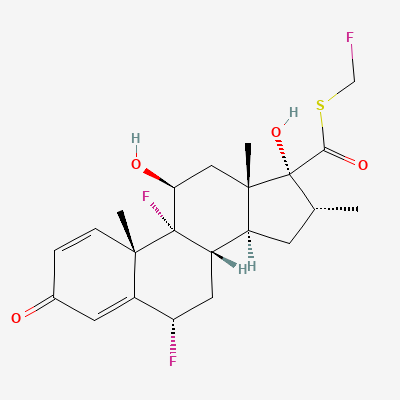
Inhaled corticosteroid (ICS) / Glucocorticoid · Corticosteroid
Also known as Fluticasone propionate, Fluticasone furoate
KDIGO 2024 + manufacturer label
144 branded formulations and 142 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
High-affinity binding to intracellular glucocorticoid receptors, translocating to nucleus where it upregulates anti-inflammatory gene transcription (lipocortin, IL-10) and suppresses pro-inflammatory gene expression (cytokines, chemokines, adhesion molecules). First-pass hepatic metabolism minimizes systemic exposure.
Compatible with pregnancy at standard inhaled doses; benefits of controlled asthma outweigh risks; use lowest effective dose
Excretion in breast milk is minimal at standard inhaled doses; compatible with breastfeeding
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Drug interaction classified as: others
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Katzung, BNF, Nelson, Harriet Lane·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19