Alfentanil
Severe
Database
Drug interaction classified as: synergy
Source: DDInter
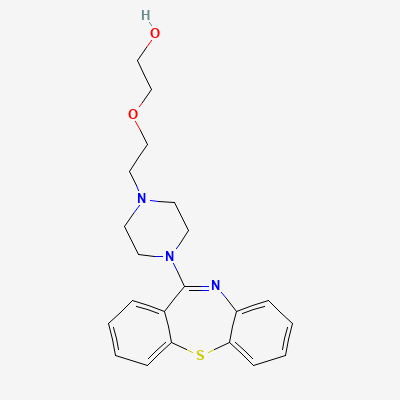
Atypical Antipsychotic · Antipsychotic
Also known as Quetiapine Fumarate, Seroquel, Seroquel XR, Q-Pin, Qutipin
KDIGO 2024 + manufacturer label
361 branded formulations. Look up specific brands in the Drugs workspace.
Quetiapine is a dibenzothiazepine atypical antipsychotic with a broad receptor binding profile. It has high affinity for histamine H1 receptors (potent sedation), moderate affinity for 5-HT2A and 5-HT1A receptors, and moderate affinity for dopamine D2 receptors (rapid dissociation from D2 — 'hit-and-run' kinetics). Its relatively low D2 occupancy compared to other antipsychotics accounts for its low extrapyramidal symptom risk. It also blocks alpha-1 adrenergic receptors (orthostatic hypotension) and has minimal anticholinergic activity. The active metabolite norquetiapine has higher affinity for norepinephrine reuptake transporters (NET), contributing to antidepressant effects.
FDA PLLR: Limited human data. Neonatal EPS and withdrawal symptoms reported with third-trimester exposure. Use only if benefit clearly outweighs risk. Risk of metabolic complications in pregnancy.
Excreted in breast milk. May cause infant sedation, poor feeding, developmental effects. Avoid breastfeeding if possible.
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18