Amiodarone
Contraindicated
Database
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
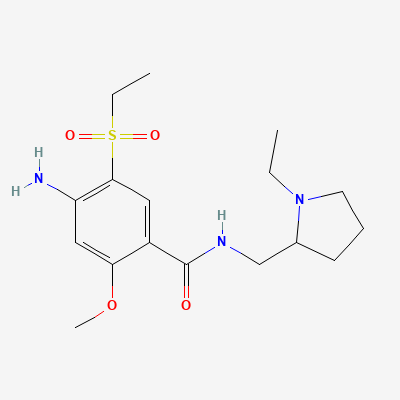
Atypical Antipsychotic · Antipsychotic
Also known as Sulpitac, Amisant, Solian
KDIGO 2024 + manufacturer label
361 branded formulations. Look up specific brands in the Drugs workspace.
Amisulpride is a substituted benzamide atypical antipsychotic with high selectivity for dopamine D2 and D3 receptors. At low doses (50-300 mg/day), it preferentially blocks presynaptic D2/D3 autoreceptors, enhancing dopaminergic transmission in the mesocortical pathway — this accounts for its efficacy in negative symptoms of schizophrenia and dysthymia. At higher doses (400-1200 mg/day), it blocks postsynaptic D2/D3 receptors in the mesolimbic pathway, reducing positive symptoms of schizophrenia. It has minimal affinity for 5-HT2A, alpha-1, H1, and muscarinic receptors, resulting in a relatively clean side effect profile with low sedation, minimal weight gain, and reduced metabolic effects compared to other atypical antipsychotics. It does not cross the blood-brain barrier extensively in areas responsible for motor control, reducing extrapyramidal symptoms.
FDA PLLR: Not approved in US (EU/India use). Animal studies showed adverse effects. Limited human data. Hyperprolactinemia may affect fertility. Use only if benefit clearly outweighs risk.
Excreted in breast milk. Hyperprolactinemia may suppress lactation. Avoid breastfeeding if possible. If necessary, monitor infant for EPS, sedation, and developmental effects.
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18