Diazepam
Severe
Textbook-cited
Excessive sedation, respiratory depression, motor impairment.
Avoid concurrent use
Source: KDT 7e · p950
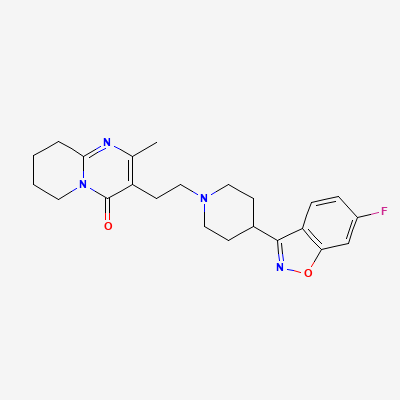
Atypical Antipsychotic · Antipsychotic
Also known as Risperdal, Risdone, Rispax, Zisper
KDIGO 2024 + manufacturer label
306 branded formulations and 193 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Risperidone is a benzisoxazole atypical antipsychotic that acts as a combined serotonin-dopamine antagonist. It has high affinity for 5-HT2A receptors (Ki = 0.16 nM), D2 receptors (Ki = 3.3 nM), alpha-1 adrenergic receptors, and H1 histamine receptors. The 5-HT2A/D2 affinity ratio >1 is characteristic of atypical antipsychotics and is thought to reduce extrapyramidal symptoms while maintaining antipsychotic efficacy. It also blocks alpha-2 adrenergic receptors and has moderate affinity for H1 receptors. Unlike clozapine or olanzapine, risperidone has minimal anticholinergic (M1) activity. Its active metabolite, 9-hydroxyrisperidone (paliperidone), contributes significantly to the pharmacological effect.
FDA PLLR: Limited human data. Neonatal extrapyramidal and/or withdrawal symptoms reported with third-trimester exposure. Use only if benefit clearly outweighs risk.
Excreted in breast milk (infant dose ~2.3-4.7% of maternal weight-adjusted dose). May cause infant sedation, EPS, poor feeding. Avoid breastfeeding if possible.
Excessive sedation, respiratory depression, motor impairment.
Avoid concurrent use
Source: KDT 7e · p950
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Exposure to active moiety increases by 1.5-fold.
Reduce risperidone dose.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18