Phenelzine
Contraindicated
Database
Serious drug interaction.
Avoid coadministration.
Source: DDInter
Opioid Analgesic · Analgesic
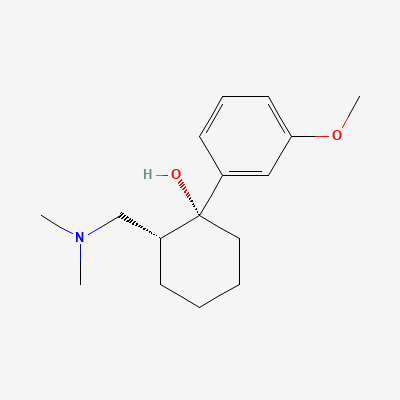
Also known as Tramadol hydrochloride, Ultram, Tramal, ConZip, Rybix ODT
KDIGO 2024 + manufacturer label
591 branded formulations and 744 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Tramadol is a centrally-acting synthetic opioid analgesic with a dual mechanism of action. The (+)-enantiomer and its O-desmethyl metabolite (M1) are mu-opioid receptor (MOR) agonists with approximately 6000-fold lower affinity than morphine. Additionally, (+)-tramadol inhibits serotonin (5-HT) reuptake and (-)-tramadol inhibits norepinephrine (NE) reuptake. These complementary monoaminergic and opioid pathways produce synergistic analgesia for moderate to moderately severe pain. The M1 metabolite is 200-300 times more potent at MOR than parent tramadol and has a longer half-life (7.4 hours vs 6.3 hours).
FDA PLLR: Can cause fetal harm and neonatal opioid withdrawal syndrome if used during pregnancy. Use only if benefit clearly outweighs risk. Avoid near term (risk of respiratory depression in newborn). Not recommended for prolonged use during pregnancy.
Excreted in breast milk (infant dose ~1-3% of maternal weight-adjusted dose). One reported infant death from tramadol exposure via breast milk (possible CYP2D6 ultra-rapid metabolizer mother or infant). Use with caution; monitor infant for excessive sedation, respiratory depression, poor feeding.
Serious drug interaction.
Avoid coadministration.
Source: DDInter
Serious drug interaction.
Avoid coadministration.
Source: DDInter
MAOIs + tramadol = high risk of serotonin syndrome and hypertensive crisis. Tramadol inhibits serotonin reuptake; MAOIs prevent serotonin breakdown.
Absolute contraindication. Do not use tramadol within 14 days of MAOI discontinuation. Choose alternative analgesia.
Source: Kimi deep-research + Cla
Increased risk of respiratory depression, profound sedation, coma, and death
Advise patients to avoid alcohol consumption while taking tramadol.
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18