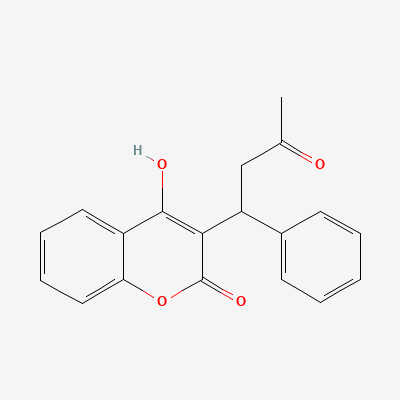
Rivaroxaban
Contraindicated
Database
Dual anticoagulation with no additional benefit but substantially increased bleeding risk.
Do not combine. Transition with appropriate overlap (start rivaroxaban when INR <3.0).
Source: Kimi deep-research + Cla
Anticoagulant
Also known as Warfarin Sodium, Coumadin, Jantoven
KDIGO 2024 + manufacturer label
17 branded formulations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Warfarin inhibits the enzyme Vitamin K epoxide reductase complex subunit 1 (VKORC1) in the liver. This prevents the regeneration of reduced vitamin K, a crucial cofactor for the gamma-carboxylation of clotting factors II (prothrombin), VII, IX, and X, as well as anticoagulant proteins C and S. Consequently, functionally inactive forms of these factors are produced, leading to a dose-dependent anticoagulant effect and prolonged clotting times.
Category X (1st trimester) → D — LMWH preferred
Warfarin is considered compatible with breastfeeding. Studies indicate minimal transfer of active warfarin into breast milk, making it safe for nursing infants. Monitor infant for signs of bleeding.
Dual anticoagulation with no additional benefit but substantially increased bleeding risk.
Do not combine. Transition with appropriate overlap (start rivaroxaban when INR <3.0).
Source: Kimi deep-research + Cla
Increased anticoagulant effect and bleeding risk.
Monitor INR and reduce warfarin dose as needed
Source: KDT 7e · p948
Elevated INR and increased bleeding risk.
Monitor INR closely; reduce anticoagulant dose if needed
Source: KDT 7e · p948
Elevated INR and increased bleeding risk.
Monitor INR closely; reduce anticoagulant dose if needed
Source: KDT 7e · p948
Significantly increased bleeding risk, especially GI bleeding.
Avoid concurrent use
Source: KDT 7e · p949
Elevated INR and bleeding risk
Avoid concurrent use or monitor INR and reduce dose
Source: KDT 7e · p948
Loss of anticoagulant effect; thromboembolic risk.
Avoid or increase warfarin dose with frequent INR monitoring
Source: KDT 7e · p949
Increased bleeding risk
Monitor INR and reduce anticoagulant dose
Source: KDT 7e · p948
Increased bleeding risk.
Monitor INR and reduce anticoagulant dose
Source: KDT 7e · p948
Significantly increased bleeding risk, especially GI bleeding.
Avoid concurrent use
Source: KDT 7e · p949
Increased anticoagulant effect and bleeding risk.
Monitor INR and reduce warfarin dose
Source: KDT 7e · p948
Elevated INR and bleeding risk.
Avoid concurrent use or monitor INR and reduce dose
Source: KDT 7e · p948
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-06-01 · House clinical team·Cockpit curated: 2026-05-16