Cladribine
Severe
Database
Drug interaction classified as: synergy
Source: DDInter
Anthelmintic
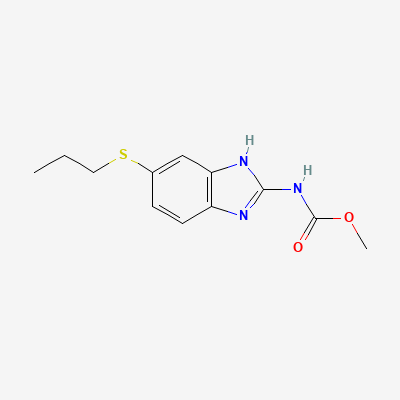
Also known as Albendazole sulfoxide, Albenza, Zentel
KDIGO 2024 + manufacturer label
852 branded formulations and 13 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Albendazole is a broad-spectrum benzimidazole anthelmintic that inhibits parasite microtubule polymerization by binding to beta-tubulin. This binding prevents the assembly of alpha- and beta-tubulin dimers into functional microtubules, disrupting cellular transport, nutrient uptake, and structural integrity of the parasite. The drug also inhibits glucose uptake by the parasite, depleting glycogen stores. Albendazole itself has limited systemic bioavailability; its active metabolite, albendazole sulfoxide (formed by hepatic flavin monooxygenases and cytochrome P450 enzymes), is responsible for the systemic anthelmintic activity.
Avoid in pregnancy (esp. first trimester) — teratogenic/embryotoxic in animals at low multiples of the human dose. FDA: obtain a pregnancy test before therapy; effective contraception during and for 1 month after. Single-dose deworming exposure has not shown increased fetal risk in published studies.
Excreted in breast milk in low concentrations. Caution advised. Consider risk-benefit. Avoid single-day therapy during breastfeeding if possible.
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Increased plasma levels of albendazole sulfoxide. In neurocysticercosis, glucocorticoids are often started before albendazole to reduce side effects from inflammatory reactions.
Glucocorticoid therapy is usually begun before initiating albendazole therapy and continued for several days after commencement of therapy to reduce the incidence of side effects resulting from inflammatory reactions.
Source: G&G 14e · p1325-1334
CYP inducers reduce plasma levels of albendazole sulfoxide by increasing metabolism, potentially reducing anthelmintic efficacy.
Monitor for treatment failure (persistent parasites). May need higher albendazole dose or alternative anthelmintic. Consider switching to non-inducing antiepileptic (valproate, levetiracetam) if feasible.
Source: Kimi deep-research + Cla
Decreased plasma concentrations of albendazole sulfoxide, potentially leading to reduced therapeutic effect.
Monitor for reduced efficacy of albendazole. Consider increasing albendazole dose if clinically indicated and tolerated, or consider alternative anthelmintic if possible.
Source: DDInter
Cimetidine inhibits metabolism and increases plasma concentration of albendazole active metabolite, potentially increasing efficacy but also toxicity.
May be used therapeutically to increase albendazole levels (e.g., for hydatid disease). Monitor LFTs. If unintended, watch for increased side effects.
Source: Kimi deep-research + Cla
Dexamethasone increases albendazole sulfoxide plasma levels by ~50% via inhibition of metabolism or displacement from protein binding. Used therapeutically in neurocysticercosis but increases hepatotoxicity risk.
Standard combination for neurocysticercosis. Monitor LFTs closely. Beneficial interaction in this context.
Source: Kimi deep-research + Cla
Grapefruit juice inhibits intestinal CYP3A4 and P-gp, increasing albendazole bioavailability and plasma levels.
Avoid grapefruit juice during albendazole therapy to prevent unpredictable increases in drug levels and toxicity.
Source: Kimi deep-research + Cla
Decreased plasma concentrations of albendazole sulfoxide, potentially leading to reduced therapeutic effect.
Monitor for reduced efficacy of albendazole. Consider increasing albendazole dose if clinically indicated and tolerated, or consider alternative anthelmintic if possible.
Source: DDInter
Decreased plasma concentrations of albendazole sulfoxide, potentially leading to reduced therapeutic effect.
Monitor for reduced efficacy of albendazole. Consider increasing albendazole dose if clinically indicated and tolerated, or consider alternative anthelmintic if possible.
Source: DDInter
Albendazole increases praziquantel plasma levels (inhibition of metabolism). Combined use enhances cysticidal effect for neurocysticercosis but increases adverse effects.
Standard combination for neurocysticercosis. Monitor LFTs and adverse effects. Ensure corticosteroid cover.
Source: Kimi deep-research + Cla
Potential for increased plasma levels of albendazole sulfoxide.
Caution is advised when using high doses of albendazole together with drugs that inhibit hepatic CYPs, such as ritonavir.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18