Atracurium
Severe
Database
Clinical effect not specified
Source: DDInter
Aminoglycoside · Antibiotic
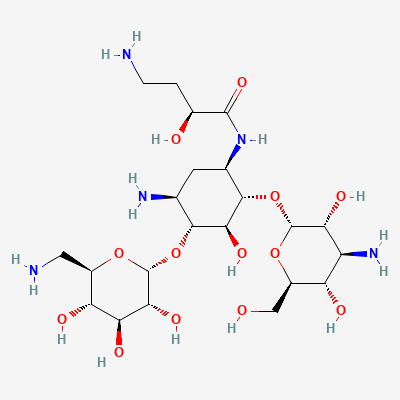
Also known as Amikacin sulfate
KDIGO 2024 + manufacturer label
1,746 branded formulations and 7 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Amikacin is a semisynthetic aminoglycoside antibiotic derived from kanamycin A. It exerts bactericidal activity by irreversibly binding to the 30S ribosomal subunit, causing misreading of mRNA and inhibition of bacterial protein synthesis. The 1-N-(L-4-amino-2-hydroxybutyryl) side chain confers resistance to most bacterial aminoglycoside-inactivating enzymes, making amikacin active against many gentamicin- and tobramycin-resistant gram-negative organisms.
FDA PLLR: Aminoglycosides can cause fetal harm. Ototoxicity has been reported in fetuses exposed in utero. Use only if clearly needed and benefit outweighs risk. Avoid if possible, especially in first trimester.
Excreted in breast milk in low concentrations. Risk to nursing infant is low but theoretical (ototoxicity, nephrotoxicity). Consider discontinuing breastfeeding during treatment or monitor infant for adverse effects.
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Increased risk of acute kidney injury and ototoxicity
Avoid concomitant use. If unavoidable, monitor renal function and auditory function extremely closely. Consider alternative antibiotics if possible during cisplatin therapy.
Source: DDInter
Clinical effect not specified
Source: DDInter
Increased risk of acute kidney injury and respiratory depression/paralysis
Avoid concomitant use due to high risk of toxicity. If no other options, monitor renal function and respiratory status extremely closely. Be prepared for respiratory support.
Increased risk of acute kidney injury and elevated cyclosporine levels due to impaired renal clearance.
Avoid concomitant use. If unavoidable, monitor renal function and cyclosporine trough levels very closely. Adjust cyclosporine dose as needed. Consider alternative antibiotics.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18