Cephalothin
Severe
Textbook
Exaggerated kidney failure.
Avoid co-administration due to enhanced toxicity.
Source: KDT 7e · p700
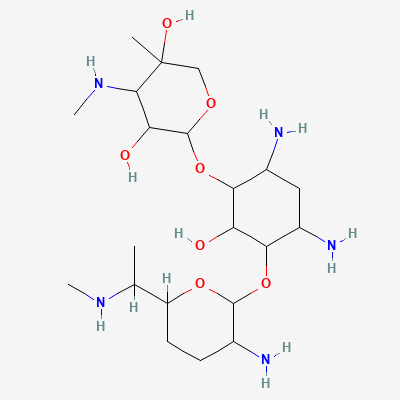
Aminoglycoside · Antibiotic
Also known as Gentamicin Sulfate, Garamycin, Cidomycin
KDIGO 2024 + manufacturer label
133 branded formulations and 224 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Gentamicin is an aminoglycoside antibiotic that exerts concentration-dependent bactericidal activity by irreversibly binding to the 30S ribosomal subunit. This binding disrupts bacterial protein synthesis at multiple steps: (1) it causes misreading of mRNA codons, leading to incorporation of incorrect amino acids into growing peptide chains; (2) it inhibits translocation of the peptidyl-tRNA from the A-site to the P-site; and (3) it blocks the initiation complex formation. The resulting aberrant proteins insert into the bacterial cell membrane, increasing permeability and leading to cell death. Gentamicin's activity is concentration-dependent — higher peak concentrations relative to MIC result in more rapid and extensive bacterial killing.
FDA PLLR: Can cause fetal harm. Ototoxicity risk to fetus (irreversible bilateral congenital deafness reported with streptomycin; similar risk assumed for gentamicin). Use only if clearly needed and benefit outweighs risk.
Excreted in breast milk in low concentrations. Risk to nursing infant is low but theoretical. Monitor infant for GI upset, diarrhea, candidiasis, or hearing problems.
Exaggerated kidney failure.
Avoid co-administration due to enhanced toxicity.
Source: KDT 7e · p700
Significantly increased risk of acute kidney injury (AKI).
Avoid concomitant use if possible. If unavoidable, monitor renal function (serum creatinine, BUN, urine output) very closely. Ensure adequate hydration. Adjust doses of both drugs as per renal function.
Drug interaction classified as: antagonism
Source: DDInter
Prolonged paralysis, respiratory failure
Monitor neuromuscular function. May need extended ventilation.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Permanent hearing loss, renal failure
Avoid combination. Space apart if both needed.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18