Apalutamide
Severe
Database
Drug interaction classified as: metabolism
Source: DDInter
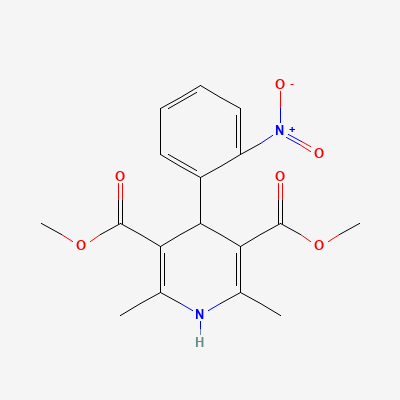
Dihydropyridine calcium channel blocker · Antihiccup agent
KDIGO 2024 + manufacturer label
75 branded formulations and 9 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Selectively inhibits L-type voltage-gated calcium channels in vascular smooth muscle, causing arterial vasodilation (much greater effect on arteries than veins or myocardium). Reduces peripheral vascular resistance and blood pressure. Minimal direct effect on cardiac conduction or contractility at therapeutic doses.
Commonly used for pregnancy-related hypertension and preterm labor tocolysis. No teratogenic effects documented. Fetal safety well-established. Preferred CCB in pregnancy (with labetalol and methyldopa).
Excreted in breast milk in small amounts (~5% of maternal dose); compatible with breastfeeding. Monitor infant for hypotension signs.
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: metabolism.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
.
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, BNF·Verified: 2026-05-19 · House clinical team·Cockpit curated: 2026-05-19