Aceclofenac + Paracetamol
Severe
Textbook
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
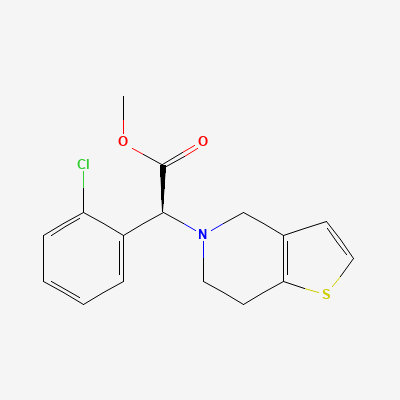
Antiplatelet
Also known as Clopidogrel bisulfate, Plavix, Clopilet, Deplatt
KDIGO 2024 + manufacturer label
213 branded formulations and 496 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Clopidogrel is a prodrug that requires hepatic activation, primarily by the CYP2C19 enzyme, to form an active metabolite. This active metabolite irreversibly binds to the P2Y12 ADP receptor on platelets, preventing ADP-mediated platelet activation and subsequent aggregation. This action effectively reduces the formation of blood clots, mitigating the risk of thrombotic cardiovascular events.
Category B — limited data, use only if essential
Animal studies indicate clopidogrel and/or its metabolites are excreted in milk. It is unknown whether clopidogrel is excreted in human milk. A decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Increased bleeding risk.
Exercise extra caution and monitor for signs of bleeding.
Source: G&G 14e
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-17 · House clinical team·Cockpit curated: 2026-05-16