Astemizole
Contraindicated
Textbook-cited
Dangerous ventricular arrhythmia (QT prolongation, torsades de pointes)
Concurrent use is contraindicated
Source: KDT 7e · p948
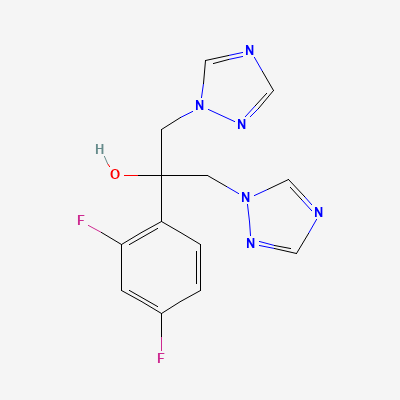
Antifungal
Also known as Diflucan, Flucostat, Flucon, Zocon
KDIGO 2024 + manufacturer label
1,350 branded formulations and 12 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Fluconazole is a synthetic triazole antifungal agent that selectively inhibits fungal cytochrome P450-dependent enzyme lanosterol 14-α-demethylase. This inhibition prevents conversion of lanosterol to ergosterol, an essential component of the fungal cell membrane. The accumulation of 14-α-methyl sterols disrupts membrane fluidity and function, increasing membrane permeability and leading to impaired fungal growth and cell death. Fluconazole is fungistatic at therapeutic concentrations but may be fungicidal against Cryptococcus and some Candida species at higher concentrations.
FDA PLLR: Low-dose fluconazole (150 mg single dose) for vulvovaginal candidiasis is generally considered acceptable in pregnancy. High-dose fluconazole (400-800 mg/day) in first trimester is associated with teratogenic effects (craniofacial, skeletal, cardiac defects). Avoid high-dose in first trimester; use only if benefit clearly outweighs risk with informed consent.
Excreted in breast milk at concentrations similar to plasma. Compatible with breastfeeding per AAP. No adverse effects reported in breastfed infants at standard doses.
Dangerous ventricular arrhythmia (QT prolongation, torsades de pointes)
Concurrent use is contraindicated
Source: KDT 7e · p948
QT prolongation and ventricular arrhythmia.
Concurrent use is contraindicated
Source: KDT 7e · p948
Dangerous ventricular arrhythmia (QT prolongation, torsades de pointes)
Concurrent use is contraindicated
Source: KDT 7e · p948
Increased plasma levels and toxicity of cilostazole.
Should not be administered along with inhibitors of CYP3A4.
Source: KDT 7e · p555
Increased pimozide plasma concentrations, leading to QT prolongation and increased risk of serious ventricular arrhythmias
Concomitant use is contraindicated. Avoid completely.
Source: DDInter
Increased risk of rhabdomyolysis and myopathy.
Avoid concurrent use; if needed, use lowest statin dose
Source: KDT 7e · p948
Carbamazepine toxicity (diplopia, ataxia, drowsiness).
Avoid concurrent use or adjust dose with monitoring
Source: KDT 7e · p948
Hypoglycemia.
Avoid concurrent use or adjust dose
Source: KDT 7e · p948
Hypoglycemia.
Avoid concurrent use or adjust dose
Source: KDT 7e · p948
Hypoglycemia.
Avoid concurrent use or adjust dose
Source: KDT 7e · p948
Increased risk of rhabdomyolysis and myopathy.
Avoid concurrent use; if needed, use lowest statin dose
Source: KDT 7e · p948
Increased risk of rhabdomyolysis and myopathy.
Avoid concurrent use; if needed, use lowest statin dose
Source: KDT 7e · p948
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18