Astemizole
Contraindicated
Textbook-cited
Dangerous ventricular arrhythmia (QT prolongation, torsades de pointes)
Concurrent use is contraindicated
Source: KDT 7e · p948
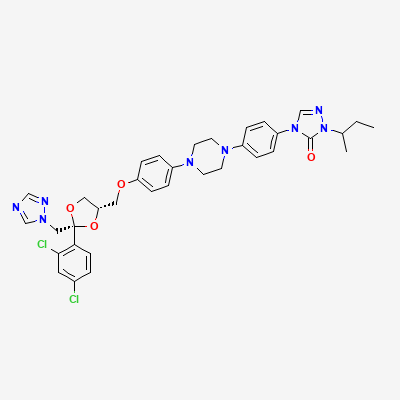
Antifungal
Also known as Itraconazole Hydrochloride, Sporanox
KDIGO 2024 + manufacturer label
2,471 branded formulations and 32 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Itraconazole is a triazole antifungal that selectively inhibits fungal cytochrome P450-dependent enzyme lanosterol 14-alpha-demethylase. This inhibition blocks the conversion of lanosterol to ergosterol, a vital component of the fungal cell membrane. The resulting depletion of ergosterol and accumulation of 14-alpha-methyl sterols disrupts fungal cell membrane integrity and function, increasing membrane permeability and inhibiting fungal growth. Itraconazole is fungistatic against most susceptible organisms; fungicidal activity may occur at high concentrations against certain organisms.
Risk cannot be ruled out. Animal studies have shown teratogenic effects (skeletal malformations). Contraindicated for onychomycosis in pregnant patients. Use for systemic mycoses only if benefit clearly outweighs risk. Effective contraception is required during therapy and for 2 months after discontinuation.
Itraconazole is excreted in human breast milk (concentration approximately 10-20% of maternal plasma). Potential for serious adverse effects in breastfed infants. Not recommended during breastfeeding. If treatment is essential, consider temporary discontinuation of nursing or use formula feeding.
Dangerous ventricular arrhythmia (QT prolongation, torsades de pointes)
Concurrent use is contraindicated
Source: KDT 7e · p948
Dangerous ventricular arrhythmia (QT prolongation, torsades de pointes)
Concurrent use is contraindicated
Source: KDT 7e · p948
Increased plasma levels and toxicity of cilostazole.
Should not be administered along with inhibitors of CYP3A4.
Source: KDT 7e · p555
Ventricular arrhythmias.
Source: KDT 7e · p795
Increased plasma levels of finerenone.
These drugs should not be administered concomitantly.
Source: G&G 14e · p570
Inducing potentially fatal cardiac arrhythmias.
Avoid coadministration.
Source: G&G 14e · p1201
Itraconazole is a potent CYP3A4 inhibitor. Cisapride is metabolized by CYP3A4; inhibition leads to markedly elevated cisapride plasma concentrations, causing QT prolongation and torsades de pointes, which can be fatal.
CONTRAINDICATED. Do not coadminister under any circumstances. If prokinetic therapy is needed, consider metoclopramide or domperidone (with caution) as alternatives.
Source: Kimi deep-research + Cla · p948
Increased domperidone plasma levels, leading to increased risk of QT prolongation and Torsades de Pointes (TdP)
Concomitant use is contraindicated. Avoid co-administration.
Ergotism
Contraindicated.
Source: DDInter
Itraconazole inhibits CYP3A4 metabolism of oral midazolam and triazolam, leading to profound and prolonged sedation, respiratory depression, and psychomotor impairment. Effects can persist for days after itraconazole discontinuation due to long half-life.
CONTRAINDICATED. Avoid concurrent use. If benzodiazepine sedation is needed, consider lorazepam, oxazepam, or temazepam (glucuronidated, not CYP3A4-dependent) as alternatives. IV midazolam may be used with caution in monitored settings.
Source: Kimi deep-research + Cla
Profound and prolonged sedation, respiratory depression.
Concomitant use of oral midazolam is contraindicated. If a benzodiazepine is required, consider one not metabolized by CYP3A4 or use parenteral midazolam with extreme caution and dose reduction.
Significantly increased plasma concentrations of silodosin, leading to an increased risk of orthostatic hypotension and other dose-dependent adverse effects.
Concomitant use is contraindicated. An alternative alpha-blocker or antifungal should be considered.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18