Celecoxib
Severe
Textbook-cited
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
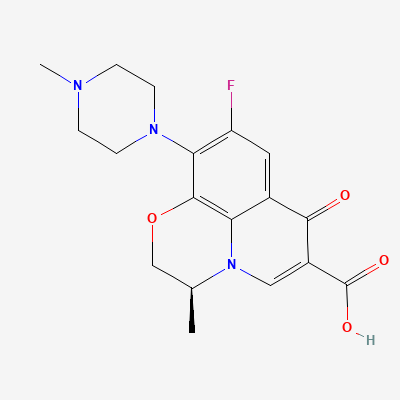
Fluoroquinolone · Antibiotic
Also known as L-Ofloxacin, Loxof, Levoquin, Glevo
KDIGO 2024 + manufacturer label
1,874 branded formulations and 299 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Levofloxacin is a synthetic broad-spectrum antibacterial agent from the fluoroquinolone class. It selectively inhibits bacterial DNA gyrase (topoisomerase II) and topoisomerase IV, which are essential enzymes for bacterial DNA replication, transcription, repair, and recombination. This inhibition leads to breaks in bacterial DNA, ultimately resulting in bacterial cell death.
Category C — avoid; arthropathy
Levofloxacin is excreted into human breast milk. Due to the potential for serious adverse effects, including arthropathy, in breastfed infants, a decision should be made whether to discontinue nursing or discontinue the drug, considering the importance of the drug to the mother. Avoid if possible.
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-16 · House clinical team·Cockpit curated: 2026-05-16