Amisulpride
Contraindicated
Database
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Fluoroquinolone · Antibiotic
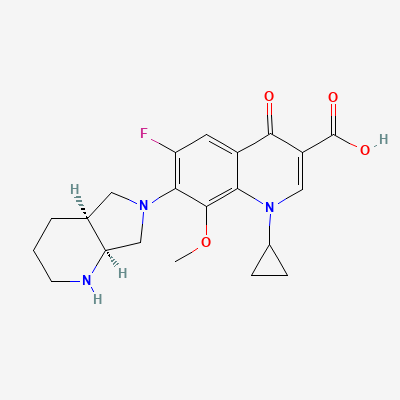
Also known as Moxifloxacin Hydrochloride
KDIGO 2024 + manufacturer label
487 branded formulations and 402 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Moxifloxacin is a synthetic fluoroquinolone antibacterial agent that exerts bactericidal activity by inhibiting two essential bacterial enzymes: DNA gyrase (topoisomerase II) and topoisomerase IV. DNA gyrase is responsible for introducing negative supercoils into bacterial DNA during replication and transcription, while topoisomerase IV is essential for partitioning daughter chromosomes during cell division. Inhibition of both enzymes prevents bacterial DNA replication, transcription, and repair, leading to rapid bacterial cell death. Moxifloxacin has enhanced activity against gram-positive organisms (including Streptococcus pneumoniae) compared to earlier fluoroquinolones due to its 8-methoxy substitution.
FDA PLLR: Avoid during pregnancy. Animal studies showed arthropathy in juvenile animals. Limited human data suggest potential risk. Use only for plague or life-threatening infections where benefit outweighs risk.
Excreted in breast milk (infant dose ~2-3% of maternal). Potential risk of arthropathy and QT effects in nursing infant. Avoid during breastfeeding. If necessary, monitor infant for GI upset, rash, and joint symptoms.
Increased risk of Torsades de Pointes (TdP) and other ventricular arrhythmias
Concomitant use is contraindicated. Avoid combination.
Source: DDInter
Severe QT prolongation and increased risk of Torsades de Pointes
Concomitant use is contraindicated due to high risk of life-threatening arrhythmias.
Source: DDInter
Additive QT prolongation via hERG potassium channel blockade. Combined use significantly increases risk of torsades de pointes and sudden cardiac death.
Absolute contraindication per FDA label. Choose alternative antibiotic (beta-lactam, azithromycin with caution) or alternative antiarrhythmic if moxifloxacin essential.
Source: Kimi deep-research + Cla
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk.
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Enhanced CNS toxicity, seizure risk
Avoid concurrent use
Source: KDT 7e · p949
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: antagonism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18