Quinidine
Contraindicated
Textbook
Fatal ventricular arrhythmias.
Avoid coadministration or ensure strict potassium management.
Source: G&G 14e · p567
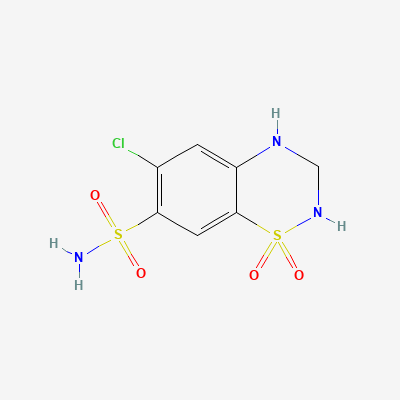
Thiazide Diuretic · Antihypertensive
Also known as HCTZ, Esidrix, Hydrodiuril, Microzide
KDIGO 2024 + manufacturer label
20 branded formulations and 87 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Hydrochlorothiazide primarily acts on the distal convoluted tubule of the nephron, inhibiting the sodium-chloride symporter. This prevents the reabsorption of sodium and chloride ions, leading to increased excretion of water, sodium, chloride, and potassium. Its antihypertensive effect is also mediated by reducing peripheral vascular resistance through unknown mechanisms.
Category B (older D) — use only when essential
Excreted into breast milk. Should be used with caution, and generally avoided if possible, especially during initial lactation, due to potential for reduced milk supply and electrolyte disturbances in the infant. A safer alternative may be preferred.
Fatal ventricular arrhythmias.
Avoid coadministration or ensure strict potassium management.
Source: G&G 14e · p567
Increased incidence of thrombocytopenia
Avoid concurrent use
Source: KDT 7e · p948
Digoxin toxicity (arrhythmias, nausea, visual disturbances).
Co-prescribe potassium-sparing diuretic or potassium supplements
Source: KDT 7e · p949
Lithium toxicity.
Reduce lithium dose and monitor serum levels
Source: KDT 7e · p949
Increased incidence of thrombocytopenia
Avoid concurrent use
Source: KDT 7e · p948
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Fatal ventricular arrhythmias.
Avoid coadministration or ensure strict potassium management.
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Fatal ventricular arrhythmias.
Avoid coadministration or ensure strict potassium management.
Source: DDInter
.
Source: DDInter
.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-16 · House clinical team·Cockpit curated: 2026-05-16